
|
Welcome,
Guest
|
Advanced Search
Search Results
| 06 Dec 2018 10:33 | |
|---|---|
|
It's fibrosis score - F0 - healthy liver, F4 - advanced fibrosis.
Done with liver ultrasound or Fibroscan in like one hour. You may actually need to know it now. On the one hand, it could be a mistake or another reason for massive liver damage: www.ueg.eu/education/latest-news/article...d-how-to-avoid-them/ The significance of aminotransferase levels in the diagnosis and prognosis of acute liver failure is often misunderstood. Excessive aminotransferase levels occur in acute viral, toxic or ischaemic liver injury. Although impressive, these levels merely reflect acute hepatocellular damage rather than loss of liver function. Consequently, marked aminotransferase elevations in the absence of jaundice, coagulopathy and encephalopathy should not lead to a diagnosis of acute liver failure. EASL recommendation: Patients with decompensated (Child-Pugh B or C) cirrhosis should be treated in experienced centres with easy access to liver transplantation and close monitoring during therapy is required, with the possibility of stopping therapy with evidence of worsening decompensation during treatment (A1). www.easl.eu/medias/cpg/2018/EASL%20Recom...8/English-report.pdf Nothing else to see here, except for the need for expert monitoring. Sof/vel is recommended for the decompensated cirrhosis but it can cause effects of decompensation (liver damage) on-treatment, when treatment should be cancelled and emergent measures should be taken. It is actually important to know your liver fibrosis state now. Read this. livertox.nih.gov/Sofosbuvir.htm Find out if you have or have had Hepatitis B or cirrhosis. If you do, it could be a serious life-threatening condition. If you don't then probably it is a test mistake. You may want to schedule other blood and liver tests corresponding to the findings of the sofosbuvir Drug Record (to confirm or exclude Hep B reactivation or hepatic decompensation). You may even need expert monitoring to assess a need for emergent liver transplantation and to see what other tests including blood tests, liver tests should be done. Or to urgently assess other test values to confirm it was a mistake. I am not a doctor at all, just would like to say that it's not okay and you should act quickly. Call ambulance, see a doctor to consult with. Do more tests. Only FDA-documented reasons related to sof+vel are Hepatitis B reactivation and cirhosis decompensation in people with cirrhosis. www.webmd.com/a-to-z-guides/aspartate_aminotransferse-test#2 Apart from the documented treatment complications, it could be additionally for one of these generic reasons or just a false positive. If you had cirrhosis or Hepatitis B, a decision to stop or continue treatment would have to be urgently made by a hepatologist in a hostipal treating people with decompensated cirrhosis. If if it is something serious, it must be fixed very soon. Or it's just a mistake/something else. But it's not okay. No such increase of AST/ALT was documented in the sof+vel FDA sheet, except for the mentioned reasons.
Category: New to Forum
|
|

{kind=link}
| 25 Jun 2017 11:19 | |
|---|---|
|
A response from the AASLD:
and
www.aasld.org/about-aasld/press-room/aas...cochrane-review-daas Edit: EASL have also responded along similar lines:
www.journal-of-hepatology.eu/pb/assets/r...chraneEASLJMP003.pdf
Category: Media & News
|
|
| 22 May 2017 19:04 | |
|---|---|
|
Hello Gert,
Yes, there are studies. You want page 18 of the EASL Guidelines (see PDF) that reports the major studies used for the guidelines and provides references for them you can then look up. SOF+VEL: ASTRAL-3 Short version: slides.hcvonline.org/uploads/194/astral3.pdf Long version: www.nejm.org/doi/full/10.1056/NEJMoa1512612#t=article SOF+DCV: ALLY-3 and ALLY-3+ Short version: slides.hcvonline.org/uploads/164/ally3.pdf Long vesion: www.ncbi.nlm.nih.gov/pmc/articles/PMC4409820/ ALLY-3+ www.ncbi.nlm.nih.gov/pubmed/26822022 There is another bigger SOF+DCV trial here: fixhepc.com/forum/gt3/369-gt3-high-svr-r...ith-daclatasvir.html which includes a PDF of the results. It does not have a funky name AFIK. 
You may notice that the results for SOF+DCV vary a bit and include similar optimistic numbers to SOF+VEL Now this table is interesting (and you won't easily find it). It comes from Abbvie who were talking about how good G/P is (previously called ABT-493/ABT-530). GS-9857 is Voxilaprevir in case you're wondering. 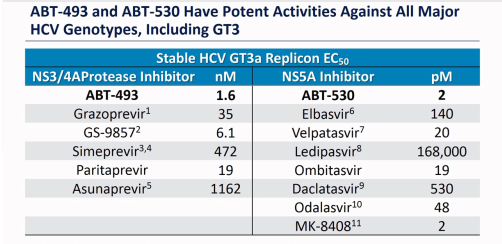
In theory Velpatasvir should be better - It has an EC50 of 20 vs 530 for daclatasvir, but only about 25% gets absorbed so that robs it of part of the 26.5x theoretical edge, dropping it to say 7x, but then the dose is 100 mg vs 60 mg so that pushes it up to about 10x. Now resistance comes in 10x, 100x and 1000x strengths so 10x is just enough to probably make a real difference for a few patients. I have no doubt that 16 weeks SOF+DCV works better in GT3 patients than 12 weeks, so that is a factor.
Category: Genotype 3 (37%)
|
|
| 03 May 2017 14:27 | |
|---|---|
|
Very good advice TM ....
SMV/DCV/SOF + RBV is one of the three retreatment options outlined in the 2016 EASL HCV Guidelines for those with GT1a who failed treatment with a regime containing an NS5a inhibitor (such as Viekira - PrOD). The other two recommended therapies are Merck's Zepatier GRZ/ELB + SOF + RBV and AbbVie's Viekira Pak PrOD + SOF + RBV. All three call for 24 weeks of therapy. Summarized in Table 9 / Page 36 www.easl.eu/medias/cpg/HCV2016/English-report.pdf I believe these EASL Guidelines became available online just after your post here. J
Category: FixHepC Admin
|
|
| 24 Mar 2017 10:44 | |
|---|---|
|
Hello again
I got back to my Doctor with your question and he said the European protocoll for treatment of the genotype 2 is Sofosbuvir with Ribavirine. He meant that the prescription is all right that way. Do you have any doubts? Should I get a second opinion? Best regards ##### Hello #####, There is nothing particularly wrong with using Sofosbuvir + Ribavirin for genotype 2. Up until the latest 2016 guidelines the recommendations were either Sofosbuvir + Ribavirin OR Sofosbuvir + Daclatasvir however.... in the new 2016 EASL guidelines (see page 17) www.easl.eu/medias/cpg/HCV2016/English-report.pdf This recommendation for Sofosbuvir + Ribavirin has been removed. The current recommendation is now either Sofosbuvir + Velpatasvir OR Sofosbuvir + Daclatasvir. So what your doctor has suggested is just a little out of date. It is no longer the recommended treatment. We have used a lot of generic Sofosbuvir + Daclatasvir in genotype 2. In fact we now have the biggest clinical trial of it ever done with 33/33 at SVR12. The reasons we chose to use Daclatasvir, rather than Ribavirin were that:
I still favour Sofosbuvir+Daclatasvir over Sofobuvir+Velpatasvir because we have very good real world data for it. With Velpatasvir being so new we really only have the drug company data to go on. It should be good, but my feeling is that it's better to stick with proven to be good at this point. I will revise that opinion if/when better data becomes available for Velpatasvir. So my suggestion would be to see your doctor again or seek a second opinion as there are much more gentle, but equally effective (probably more effective) options now recommended by the experts at EASL. Kind Regards Dr James Freeman
Category: Experts Corner
|
|
| 01 Nov 2016 01:05 | |
|---|---|
|
Summary of trials data to help one compare sof/vel with other effective treatments
congress-ph.ru/common/htdocs/upload/fm/g.../2016/prez/1-3-2.pdf www.natap.org/2016/AASLD/AASLD.htm In-vivo resistance analysis (sof/vel, all phase III trials). Enough statistics for some genotypes. www.natap.org/2016/EASL/EASL_15.htm
Category: FixHepC Admin
|
|
| 08 Oct 2016 17:39 | |
|---|---|
|
This may be helpful:
www.easl.eu/medias/cpg/HCV2016/English-report.pdf BTW What kind of retreatement are you going to follow now?
Category: Experts Corner
|
|
| 07 Oct 2016 20:13 | |
|---|---|
|
I had watched this before and did not hear the advice that these recommendations can be downloaded, I assume in pdf form.
I expect that having this document to hand when seeing your G.P. or specialist would help the conversation - a LOT. Just a suggestion that may head off any WTF moments. J.
Category: Experts Corner
|
|
| 29 Aug 2016 08:43 | |
|---|---|
Thanks, Yes, early trial, small cohort and no placebo. I went and had a quick look at just the diarrhoea results for Vox trials I could quickly access and the figures are all over the place. NCT02378935 was 9.6%, NC02378961 was 22.7% Both were non placebo trials. Interestingly I found an (admittedly phase 1) trial that used placebos NCT02185794. The placebo arm had 12.5% whereas the drug arm was only 5%. The problem with quoting small scale trials which contain no placebo arm like you did is that anytime that you get a group of people together for a period of say 12 weeks and ask them to report adverse events, diarrhoea and nausea are going to show up fairly regularly whether those people have HCV or not and whether they are taking drugs, placebo or nothing at all. They are really common symptoms of everyday life that vary from location to location and season to season so you do need to be extremely cautious about attaching significance to them particularly if there is no placebo arm to the trial. I would also suggest you reconsider your "no sides for vel" statement. See p91 (onwards) below which shows them plus whether they were considered relevant. This is why we need placebo arms, to determine whether reported sides are related to the drugs or coincidental. www.ema.europa.eu/docs/en_GB/document_li...4210/WC500211152.pdf
Category: FixHepC Admin
|
|
| 28 Aug 2016 23:00 | |
|---|---|
|
The data is preliminary (from Stage 2 trials), but Gilead announced that sof/vel/vox is 99% effective for previous DAA failures of the studied classes (without naming the classes).
Source: GILEAD announcement on EASL Conference in April. It is also widely known that vox causes diarhea and is otherwise bad for your stomach in the short term. (See links below). The data is from Stage 2 trials. So for retreatment of DAA-failures vox is a much much more effective option than say vel+sof for 24 weeks or with ribavirin. Vel is not good for retreament. It is recommended for treatment-naive people. Because it has almost no side effects and although there's no data yet if sof/vel/vox is effective for sof/vel relapsers, it is likely that this data is going to be available in the beginning of 2017. If sof/vel/vox indeed proves effective against vel-resistant viruses, there's more probability to get cured if you do, say, sof+vel and if it doesn't work you do sof/vel/vox. Because sof/vel won't bring in any NS3 mutations and there's no data on retreatment of sof/vel/vox failures yet. That said, if you're treatment-naive, get sof/vel. If DAA-experienced, wait a little. No data on if vox would help and in what situations it would (after which treatment regimens, in which liver conditions), but Stage 2 shows it is effective. regist2.virology-education.com/2016/12co...ion/21_Sulkowski.pdf www.natap.org/2016/EASL/EASL_31.htm The problem is though, vox is not going to be available until mid-2017. It is effective in cirhotic populations.
Category: FixHepC Admin
|
|
| 18 Aug 2016 09:30 | |
|---|---|
|
Not sure where to put this.... here will do. I was very pleased with this quote from the New Zealand Hepatitis Foundation's recent publication talkinghepC , Winter 2016, p7 and I think it is a really good endorsement beyond NZ, a kind of international reference, and contains useful information, so I typed it up... here it is pasted in, can be copied and pasted for use anywhere, also have attached as a full page sort of noticeboard/poster “What if I do not qualify for the funded treatment?” Personal Importation, NZ Hepatitis Foundation Clinical Director Alex Lampen-Smith discusses: “In the 2016 Autumn edition of talkinghepC, we discussed personal importation as a means of accessing affordable generic versions of the lifesaving DAA’s. Many people in New Zealand have personally imported treatment. In April 2016 Dr James Freeman, of the FixHepC Tasmanian Buyers’ Club, received a long-standing ovation following his presentation at the EASL conference in Barcelona, which presented the high cure rates, (>90 per cent) of cheaper generic medications. The international liver specialist community recognises the way in which he is helping make generic DAAs available for sufferers of hepatitis C at a fraction of the cost: the approximate cost of 12 weeks of treatment is $2500 (NZ) . If you are interested in personally importing treatment please ask your GP to refer you to a specialist for assessment to ensure you import the correct combination and length of treatment”.
Category: Media & News
|
|
| 17 Jul 2016 05:57 | |
|---|---|
|
Hello Everybody,
This message is a special one for me as today I took my last pill from the 12 weeks HCV treatment that I had. Somehow I've preferred to wait to reach the EOT in order to share my story, I guess mainly because of an unknown superstition that I had. So here it is: First of all I would like to warmly thank to my 2 Angels: Greg Jefferys and dr. Freeman. They both supported me with useful information about HCV generic medication, encouraged me to take the treatment (yes, I was initially afraid that generic drugs might be fake or poison ") ) and to get the medication (@Greg: not sure if you will ever read this, but THANK YOU VERY MUCH!!")! ) and to get the medication (@Greg: not sure if you will ever read this, but THANK YOU VERY MUCH!!")!Also many thanks to all of you who posted messages on this forum! I see you as true friends and sharing your knowledge, experiences, believes and hopes helped me a lot in the medical journey that I made 1) Before HCV I was born in Romania and I had my childhood during the communist times when children in schools were vaccinated using the same syringe (yes, one syringe used for a class having +30 pupils. Only the re-used and sterilized needles were exchanged after every child was getting the vaccine). Also in my childhood, with similar re-used syringes I was getting some rabies injection (I was bitten by a dog on the street). In the '90s, immediately after the Romanian revolution, I went for some dental works in a couple of private dental offices where I am not sure how well the instruments were sterilized. No drugs, no blood transfusion, no risky sexual practices, no piercing, no tattoos. I was very often asked these questions, so I prefer to specify this in advance. How did I got HCV? I do not know, but the aspects mentioned before offer some hints about the possible causes. Anyway, once you have HCV, I am not sure at what purpose does it serve to know how you got it, except for helping others know how to prevent getting HCV. And of course, for statistic purpose! I preferred to write this piece of information having in mind that some people, many I think, still tend to put a stigma on HCV patients. They shouldn't and neither should they judge a person because of having HCV. 2) HCV diagnosis. I was diagnosed with Hep C 13 years ago. At that time I had no idea what hepatitis C meant. I knew about hepatitis A, so... I hoped initially that hepatitis C was easier to treat because it had the letter "C", which is after the letter "A"... I was clarified asap I should not have such hopes... And so in 2003 I applied for the interferon treatment. I was told I should wait perhaps one or several years, because the waiting list was quite high, so I waited 5 years till 2008. I was never getting a clear answer about my application for the treatment, but in 2008 I was informed that my application was lost, therefore I applied again and waited "only" another 2 years. I started the interferon + ribavirin treatment in 2010. It wasn't easy, I experienced the “typical” wide range of side effects, yet I was able to finish it. I was slow responder (UND only after 6 months of treatment), and relapsed soon after EOT. I applied again, this time for the new “triple” therapy (IF+RIB+Boceprevir) and now, 5 years later, I am officially still on the waiting list. The triple therapy is no longer being provided, and I do not qualify for the newest interferon-free treatment. Officially I am in a pending status, but in my eyes, practically I've been rejected. In all this time that I waited, I was quite “active” in finding ways on how to protect my liver: maintain my energy, balance what I eat, supplements, healthy fruits, doing sport, few alcohol (i.e. occasionally drinking 1 beer or 1 glass of wine, against my dr. recommendation...). I still question myself today, why I was not acting differently in order to get cured sooner ? Could I have done something in order to avoid waiting so many years. For this question I usually give myself 2 answers, so I guess the right one is any of them or a mixture o both: - I was acting and thinking like a goose, neglecting the reality around me and the medical system; - I was having FEAR that if I will be too insistent or too demanding regarding my rights as a health insured person, I would upset some bureaucrat who might decide to not sign the paper that would allow me to get treated. And the number of people who have to sign the papers is quite significant. Perhaps it sounds silly, but remember that Romania was a former communist country, so 10-13 years ago, people were still not so much aware of having rights. And with the thousands of sick people on the waiting lists....and the stigma ….. and the “inherited” way of thinking that “the one who talks too much must be punished”... all these are answering to my question. 3) Getting to know about the new interferon-free drugs produced in India and Egypt First time I heard about it was in the summer of 2015 by reading an article about the treatment costs of 1000$ in India and many many thousands of Euros in Romania. It was not specified how this wonder drugs were commercially named, so I was kind of blind. I was frustrated about this, but I could not do anything or better say, I was not knowing what I could do. The article was this one www.hotnews.ro/stiri-esential-20178127-c...uvernul-romaniei.htm → where in the comments area you may see a recent comment about dr. Freeman's presentation from EASL :D :whistle: . For Romanian speaking people, they will see that there were a lot of comments in May and June 2015, none about how to get the generic drugs and then nothing till Jan.2016 [1 comment] and then May 2016 [1 comment]  . Please see also the bold text where ANM (The National Agency for Medicines) says that “WE CANNOT AFFORD TO DRAW A REASONABLE CONCLUSION ABOUT THE EFFICACY OF THE NEW MOLECULES”. That really locked me. Is this is cure or not. Could I get it? That was my hope. But my hopes vanished when I was told that in Romania it is not accepted as cure and that I have to have patience... And so I entered in a passive status. And being demotivated. . Please see also the bold text where ANM (The National Agency for Medicines) says that “WE CANNOT AFFORD TO DRAW A REASONABLE CONCLUSION ABOUT THE EFFICACY OF THE NEW MOLECULES”. That really locked me. Is this is cure or not. Could I get it? That was my hope. But my hopes vanished when I was told that in Romania it is not accepted as cure and that I have to have patience... And so I entered in a passive status. And being demotivated.From the medical system in RO I was constantly getting the same message: "there are new and effective treatments now, but you need to wait. Hopefully in 1-2 years you will access the treatment". I was hearing this same message in the last 5 years and that meant to me only one thing: waiting indefinitely. 4) Getting the HCV generic treatment In January this year, a friend of mine talked with her doctor about my case. She was living in a developed european country and her doctor knew about the new HCV drugs like Harvoni or Viekira. This doctor proposed to my friend to tell me that I could call him. Even though I was hesitating, I made the phone call and it was one of the best phone calls I ever made. The doctor asked me to make the blood tests that we all now know it must be done for the DAA treatment: a genotype analysis, a viral load, a fibroscan and the usual blood tests. I had to pay for this with my own money, approx. 300$, which in Romania is a significant amount of money, but I had no choice, as the Romanian NHS (known as CNAS) does not provide these blood tests so easily. With the results of my blood tests (HCV genotype 1b - this seems to be the genotype that most patients from Romania have) I called back the doctor and so he let me know about Harvoni and gently "pushed" me to get the treatment NOW as my liver was still in a good shape. But HOW to get it was the main question. Nevertheless I started to search about Harvoni, because of its 1 tablet/day regimen and so I discovered the blog of Greg Jefferys and read about his trip to India. At that time I was not sure whether I could trust Greg. In parallel, in my searches I was seeing also a lot of links pointing to fixhepc.com, which I feared initially it was a scam, because everything I was reading pointed that it was way too simple to get the treatment by compare with the bureaucracy I knew from the national healthcare system (@Dr. Freeman: perhaps if you could make the acceptance criteria in the REDEMPTION trials more complicated, maybe more patients will enroll  ..... Just kidding ). I was planning also to go to India, but …. that's a big country. Where should I go to see a doctor? I started to write e-mails to several hospitals from Mumbay, New Delhi, Chennai and some online pharmacies. Some answered me, some not. In the end I decided to contact both, Greg Jefferys and to send also an e-mail to Fixhepc (asking whether they could test for me 1 pill from the drugs I was intending to order from an on-line pharmacy). From that moment further, I got quick and solid support from Greg and dr. Freeman. ..... Just kidding ). I was planning also to go to India, but …. that's a big country. Where should I go to see a doctor? I started to write e-mails to several hospitals from Mumbay, New Delhi, Chennai and some online pharmacies. Some answered me, some not. In the end I decided to contact both, Greg Jefferys and to send also an e-mail to Fixhepc (asking whether they could test for me 1 pill from the drugs I was intending to order from an on-line pharmacy). From that moment further, I got quick and solid support from Greg and dr. Freeman.So, I've learned how I could get the generic treatment from India, how easy (in terms of legislation) it is to have it shipped to Romania, but also that it is important to have the support from my local doctor in Romania. So my next 2 challenges were to have the money and to get the receipt from my doctor. The money aspect was quite fast solved with my family's support. For the doctor's receipt, I got very useful information from dr. Freeman that I presented to my doctor and so he decided to support me an gave me the receipt for the active substances (sofosbuvir + ledipasvir). Here is a tip that I learned: I do not see quite a good idea to just go to your doctor and ask him/her to simply write a prescription for the HCV generic medication! Please consider the followings: - Inform your doctor about what you know about the HCV generic medication perhaps you might want to use this press release from ILC Barcelona 2016 ilc-congress.eu/low-cost-generic-direct-...randed-formulations/ and translated in the romanian language here fixhepc.com/media/kunena/attachments/206...lease-GenericHCV.pdf or this article written by dr. Freeman and dr. Hill onlinelibrary.wiley.com/doi/10.1111/liv.13157/pdf and translated in the romanian language here fixhepc.com/media/kunena/attachments/206...iC-no_ini_layout.pdf , or various information from medical journals where the active substances are presented, etc. - inform your doctor from where you are going to purchase the drugs. Have in mind that not only you, but also your doctor is concerned about the supply chain from where you are going to take the medication. - In the end, in this journey it is good to make team with your doctor. But ... if your doctor rejects you or if the doctor is unable to propose you a clear treatment option, then seek an alternative. Other specialist perhaps (?!?). As long as a cure exist and it is affordable to you, it's your chance to get treated. Treat now before it is too late. Going back to me, receiving the medication was more a question of waiting ~5 days to have it delivered. The most "difficult" thing was to wait those days as I was no longer having patience. 5) Getting treated - one tablet a day, 12 weeks. Simple, I really do not have much to say about it. I used the alarm clock from my phone to ring every day at 10:00 o'clock in the evening to remind me to take my pill. I also used a small calendar sheet where I marked with a cross every day when I took the pill. It proved to be a good practice for me as there were days when I was forgetting that I have to take the pill, so my "phone friend" reminded me every time. In the first 3 weeks I had some headaches and insomnia, but now, looking back, I tend to believe there was a dependency relation between my headaches and my emotional status, having still some doubts and being worried if the drugs really work. After 3 weeks and 5 days I had a VL blood test made and the result was UND. I hope it will stay like this forever. The last 8 weeks went without any other side effect. How i feel now? In one word, I feel as being cured! And with all benefits that being cured brings, yet feeling like a normal person. Months / years ago I thought that being cured must feel like having a kind of superhuman powers (a kind of Superman, Spiderman, Captain America), but now I see that I did not gain such powers.... I found my peace, I am more calm, I sleep better, I can work more, my mind is clear, I eat slightly more and I enjoy sitting and talking with my friends (which I did also in the past, but required some efforts from my side). And... I no longer feel this pressure that my clock is ticking. I am heading now to SVR12 and I hope to reach it !!! 6) A word about activism I remind here again that I am living in a former communist country where until ~25 years ago freedom of speech was a dream and having your own ideas was very often "rewarded" in a negative way. Sometimes I believe we still have a long way to go until we will really be able to talk freely. Until starting the treatment, all I knew very few about activism. I was not understanding why some people would put a plate in front of their chest with some text written on it or why some others are always in a continuous battle. Now I have a different and better view. And although activism occurs under various forms and at different levels, I think we can agree that in large, there is violent and non-violent forms of activism. My belief goes for the non-violent one. The simple message to spread about HCV treatment, and here I quote dr. Freeman, is "Generic works" (see here at 9min30sec ) . Starting from this message, other information can be added, so it is up to to each person to decide how, where, when and to whom this simple message will be communicated. In the last 12 weeks I noticed a pattern regarding the behavior of the people getting treated with generics (I hope I am not wrong – but if I am wrong, please correct me): - at the beginning there is the "anger" because of the barriers that were faced when trying to get treated through the NHS system; - then this anger combined with the new knowledge about generics leads to activism in order to help other people. It is this activism that boosts the process of spreading the news about the effective treatment with generics. - by getting closer to the EOT or after EOT, the activism turns into a kind of wisdom, wisdom about how to better help others. At this stage, some might say that people, who got already cured, no longer care about HCV patients and become passive. I would really question this. A former patient who got cured will always be an activist and will always tell to others how he/she got cured via generics. And although one person can become limited in his/her activism actions (in the end, human beings are limited beings), activism can increase with the contribution of each one of you. So have in mind that whenever you spread such news there will be, sooner or later, someone on this planet who will benefit from your information and so you will have saved one or more lives. If one stays passive, the only life that will be saved will be the own life.... I end this post with couple of points I learned in this journey: - Fear is normal. The fear made me search for information, made me behave cautious, made me get in contact with people I did not knew and get useful information. Without fear I would have probably remained untreated and..... perhaps a “goose” being sick. - Having doubts and worries is also normal - I had many, but they are not to be mentioned in this post, perhaps it makes sense to make a separate thread or to simply leave them as they are. Some worries and doubts are gone (the problem was solved), but some are still present (is there any virus hidden somewhere....??) and some new worries came in. It is funny to think that once a worry is gone, another one takes its place. Isn't life beautiful (just kidding)? In fact what I learned is that it is reasonable and normal to have worries. I also learned (again) to not give up just because I have doubts, rather it pushed me to search for more information. My mood, during the searches I made, oscillated very much between extremely negative to extremely positive, back to negative, then back to positive, and so on...But all this swinging had a good outcome, it helped me to make my choice based on the information I collected and analyzed. It was THE CHOICE! So, that's my story... I wish you all the best, safe journey to SVR12 for those who will start it or are currently on route to get cured and hopefully we will all meet after the SVR12 line. Cheers, RHF
Category: End of Treatment - EOT
|
|
| 23 Jun 2016 07:07 | |
|---|---|
|
Incarc in aceasta postare traducerea in limba romana a articolului "Utilizarea medicamentelor generice pentru hepatita C" scris de Dr. Freeman si Dr. Hill si publicat in Liver International in sectiunea "Dezbateri in Hepatologie"
Herewith I am uploading the Romanian translation of the article "The use of generic medications for hepatitis C" written by Dr. Freeman and Dr. Hill and published in Liver International in the section "Debates in Hepatology" Utilizarea medicamentelor generice pentru hepatita C activitatea de traducere a fost efectuată în regim de voluntariat de către un utilizator înregistrat pe platforma fixhepc.com. Deși traducătorul a depus cele mai bune eforturi pentru a furniza o traducere de acuratețe ridicată, acesta nu își poate asuma responsabilitatea asupra ei, în caz de dubii ori în scop de clarificare, textul original, în limba engleză, putând fi consultat la adresa sursă: fixhepc.com/media/kunena/attachments/391/LiverInternational.pdf James A. D. Freeman1 și Andrew Hill2 1 GP2U Telehealth, Hobart, Tas., Australia 2 St Stephens AIDS Centre, Chelsea and Westminster Hospital, London, UK Abstract La nivel mondial, hepatita C, hepatita B, HIV, TBC și malaria sunt cele cinci cauze majore de deces din boli infecțioase. Printr-o descoperire care rivalizează cu inventarea penicilinei, au apărut pe piață medicamente care vindecă hepatita C cu efecte secundare minime și cu rate ridicate de succes, dar, în ceea ce trebuie să fie una dintre cele mai mari tragedii ale timpurilor moderne, aceste medicamente salvatoare nu sunt utilizate la scară largă. Brevete farmaceutice sunt dăruite corporațiilor private de către guverne în dublu scop, de protejare a cheltuielilor pentru cercetare și dezvoltare și de încurajare a inovației. Din păcate, puterii de stabilire a prețurilor de monopol pe care aceste brevete o oferă îi lipsesc măsurile de verificare și echilibrare adecvate, este deschisă la abuz, și este destul de clar că se abuzează. Tipul de modificări legislative, necesare pentru a se furniza în baza scopurilor inițiale ale brevetelor farmaceutice, vor dura ani sau chiar decenii pentru a avea loc. Importul paralel de medicamente generice oferă speranță pentru milioanele de pacienți cu HCV ce nu își permit să acceseze mult prea scumpele medicamente inovatoare. Medicii care prescriu și monitorizează pacienții care iau generice se pot simți confortabil din faptul că rezultatele studiilor REDEMPTION arată, precum anterior cu genericele pentru HIV, că medicamentele generice HCV dau rezultate clinice robuste. Puncte cheie • Inventarea medicamentelor DAA ar trebui să fie un motiv de sărbătoare la nivel mondial, deoarece aceasta oferă puterea de a salva milioane de vieți și, practic, de a elimina una dintre cele cinci cauze majore de deces din boli infecțioase. • Din păcate, pentru majoritatea pacienților, aceste medicamente inovatoare rămân inaccesibile. • Dovezile privind siguranța și eficacitatea clinică a genericelor HCV este convingătoare. • Utilizarea importului paralel de medicamente generice oferă o soluție imperfectă, dar pragmatică pe termen scurt, cât timp cadrul legislativ se reechilibrează. • În cazul în care tendințele actuale de stabilire a prețurilor farmaceutice sunt lăsate să continue, sistemul nostru de asistență medicală va deveni din ce în ce mai inaccesibil. Context Companiile farmaceutice operează într-un mediu de piață puternic subvenționat și protejat. Într-o afacere obișnuită, o companie investește în cercetare și dezvoltare, dezvoltă produse pe care le vinde apoi la prețuri pe care consumatorii și le pot permite, și, dacă aceste produse sunt populare, obțin profituri frumoase. Companiile farmaceutice operează mult în afara controlului normal al prețurilor, făcând produse pe care consumatorii individuali nu și le pot permite și sunt puternic subvenționate din fondurile publice finanțate de cetățeni prin banii din taxe și asigurări medicale. Brevetele farmaceutice sunt o completare relativ nouă la peisajul protecției proprietății intelectuale, și multe rapoarte detaliate s-au scris despre amândouă și despre problemele cu privire la puterile de monopol pe care acestea le oferă(1-3). Argumentul pentru brevetele farmaceutice este de a se încuraja cheltuielile de capital cu risc ridicat pentru cercetare și dezvoltare și, prin urmare, să se livreze pe piață produse noi, inovatoare, fiind sigur că investițiile de capital de risc, necesare pentru a face acest lucru, sunt protejate printr-o garantare a drepturilor exclusive de comercializare și a profiturilor ulterioare. În fine, aceasta este doar teoria. Întrebarea cheie este: Primim noi, cetățenii contribuabili, o valoare bună pentru banii noștri, din taxe și asigurări, câștigați cu greu? Eu susțin că brevetele farmaceutice, așa cum sunt ele în prezent, eșuează în datoria față de lume și nu oferă ceea ce este necesar. Multe cifre sunt citate, în ceea ce eu numesc ficțiune atent lucrată, pentru a întreține starea curentă. Sunt sigur că sunteți familiarizați cu ele: este nevoie de 10-15 ani pentru a aduce un medicament pe piață, doar 1 din 10 medicamente reușește și costurile pentru dezvoltarea medicamentelor noi depășesc 1 miliard$ Un articol cu impact subtanțial a fost publicat în Jurnalul Medical Britanic în 2012 (4) și conține observații ce demontează multe mituri: 1 Contrar afirmațiilor că descoperirea de medicamente noi costă 1.3 miliarde $, cifră avansată de Tufts Center, care este sprijinit de industrie, la o analiză mai amănunțită costul real este de 90-300 milioane $. 2 Modelul de afaceri farmaceutice se bazează mai degrabă pe exploatarea protecțiilor guvernamentale împotriva concurenței pieței libere decât pe descoperirea de noi medicamente. 3 Companiile farmaceutice cheltuie de 19 ori mai mult pe marketing (25% din încasări) decât pe descoperirea de noi medicamente (1.3% din încasări). 4 În timpul perioadei de 15 ani, din 1995 până în 2010, costurile R&D au crescut la 34.2 miliarde $ în timp ce veniturile au crescut de 6 ori mai rapid, la 200.4 miliarde$. Pe scurt, companiile farmaceutice cer acum cu mult mai mult profit pentru aceleași cheltuieli ca acum 20 de ani în urmă, iar acest lucru se reflectă în prețurile astronomice pentru noile medicamente inovatoare. Problema pentru societate în general este că această lăcomie sufocă gâsca ce face ouăle de aur, și dacă tendințele actuale vor continua, sistemele noastre de sănătate se vor prăbuși în cele din urmă sub greutatea costurilor tot mai mari. Pentru a face situația și mai dureroasă, companiile farmaceutice sunt totodată foarte eficiente în a evita plata impozitelor. De exemplu, Bloomberg a publicat un articol cu titlul Gilead Evită Plata Taxelor de Miliarde US $ pe medicamentul său de 1.000$ per pastilă (5). Sofosbuvir ca exemplu Sofosbuvir este o medicație inovatoare și pilonul celui mai popular dintre noile regimuri DAA pentru HCV. Putem obține o evaluare foarte exactă a costului său de dezvoltare, deoarece sofosbuvir nu a fost de fapt dezvoltat de către Gilead Sciences. Sofosbuvir a fost dezvoltat și adus în Faza a 2-a a studiilor clinice de către Pharmassets, companie listată la bursa NASDAQ. Datele contabile ale Pharmassets, de la înființarea în anul 2001 până la achiziționarea ei de către Gilead în 2011, sunt publice permițând o cuantificare foarte precisă a costurilor reale de dezvoltare ale acestui medicament. Costurile de dezvoltare la Pharmassets au fost 281 de milioane $ (6). Faza a 3-a a studiilor clinice efectuate de Gilead au avut riscuri relativ scăzute având în vedere rata de mortalitate atât a bolii cât și a tratamentelor existente atunci, și ar fi adăugat mai puțin de 125 milioane $ la totalul costurilor, luând în calcul dimensiunile documentate ale studiului în faza a 3-a, de 982 pacienți pentru Sovaldi ( 6), 1952 pacienți pentru Harvoni (7) și un cost per pacient de 42 000 $ ( ") . În 3 ani de la lansarea sa, franciza Sovaldi a adus 31.5 miliarde de dolari în venituri (9). . În 3 ani de la lansarea sa, franciza Sovaldi a adus 31.5 miliarde de dolari în venituri (9).Deși nu este în totalitate nerezonabil că investitorii în Pharmassets ar trebui să se bucure de venituri ridicate pentru plasarea de capitalul de risc, Gilead ține lumea captivă prin preț și acces, și făcând în fiecare an mai mult decât investiția sa inițială de 11 miliarde $ dolari. Este trist să te gândești la faptul că mai mulți sunt oamenii care au murit de HCV anul trecut, aproximativ 500 000 de oameni, decât cei care au primit tratamentele noi (3, 10, 11). Stabilirea prețurilor în baza valorii Sistemul nostru actual de stabilire a prețurilor bazat pe valoarea este, de asemenea, o problemă. A fost introdus pentru a încerca și controla prețurile, dar a fost reconvertit în mod eficient de către companiile farmaceutice. Răspunsul standard al lui Gilead cu privire la prețul extraordinar al medicamentelor sale este "Noi credem că prețul Harvoni reflectă valoarea medicamentului" (12). Problema fundamentală a acestui mod de gândire este că, atât timp cât se menține, vom vedea medicamente inovatoare, dar nu vom vedea niciodată îmbunătățiri ale prețurilor. Fără să se îmbunătățească prețurile, beneficiul net al medicamentelor inovatoare va fi de aproximativ zero, în ceea ce privește sănătatea la nivel mondial. Noi plătim pentru ea prin banii de taxe și de asigurări și avem dreptul de a cere mai mult. Analogia mea ar fi că, dacă Gilead ar fi inventat e-mail-ul, un "Gmail" ar avea un preț de 0,90$ bazat pe faptul că este mai ieftin decât un timbru de 1$, și oferă mijloace de urmărire și de livrare instantanee. Imaginați-vă o lume fără schimbarea majoră a prețului performant oferit de e-mail. Cât costă sofosbuvir în realitate? Deși ingredientele pentru un tratament de 12 săptămâni cu Sovaldi costă mai puțin de 100$ (13), prețul de vânzare cu amănuntul din SUA este de un uimitor 84 000 $ (fig. 1). Pentru a pune acest preț în perspectivă, în cazul în care Apple ar pune aceeași majorare de 100 000%, un iPhone nou ar costa 1 milion de dolari. 
Fig. 1. Prețul de vânzare cu amănuntul pentru Sofosbuvir în tările selectate din întreaga lume. Generice, licențe voluntare de medicație și licențe obligatorii Medicamentele generice sunt copii aproape identice ale medicamentelor brevetate originale și servesc mai multe scopuri. La expirarea brevetelor farmaceutice, capacitatea de a produce copii generice duce rapid la o scădere a prețurilor, de exemplu, Viagra a fost o pastilă de 20$ cât timp era sub brevet, iar acum este sub 4$, din cauza concurenței de preț cu cele generice. Țărilor mai puțin dezvoltate (LDC) le este permis în conformitate cu prevederile acordului Organizației Mondiale a Comerțului (OMC), privind aspectele comerciale ale drepturilor de proprietate intelectuală (TRIPS), să producă medicamente brevetate pentru propriul lor uz intern, precum și pentru utilizarea în alte țări mai puțin dezvoltate (LDC). Țările cu venituri mici și medii (LMICS) sunt uneori capabile să negocieze licențe voluntare cu producătorul, și în cazul în care aceasta nu este posibilă, licențierea obligatorie (de fapt ignorarea brevetului) este o opțiune pentru medicamentele din lista OMS a medicamentelor esențiale (14), cu toate acestea, în special SUA, nu ezită cu privire la aplicarea de sancțiuni comerciale țărilor care exercită acest drept (3,15). Legalitatea și moralitatea folosirii genericelor pentru a ocoli brevetele și prețurile excesive Trebuie să recunosc că m-am luptat foarte mult cu acest lucru, dar l-am rezolvat după cum urmează. Este corect din punct de vedere moral să lovești pe cineva în cap cu o bâtă de baseball? În mediu izolat, nu, dar: Este corect din punct de vedere moral să lovești pe cineva în cap cu o bâtă de baseball dacă ține un pistol la capul altcuiva? Pentru mine, răspunsul este da, pentru că este cel mai mic dintre două rele. Lumea este ținută captivă prin prețurile farmaceutice și la fel ca tâlharii unei epoci apuse, companiile farmaceutice cer "banii tăi sau viața ta". Cu sistemele noastre de sănătate deformate sub presiunea creșterii continue a prețurilor, sugerez că trebuie să trimitem un mesaj ferm către companiile farmaceutice despre așteptările noastre că sunt necesare profituri rezonabile și un acces al pacienților la scară largă. După cum legalitatea tehnică duce la faptul că brevetele oferă drepturi de monopol, care sunt deschise la abuzuri, cu toate acestea, alte legi dau alte drepturi. Articolul 60 din Acordul TRIPS al Organizației Mondiale a Comerțului aplică o scutire pentru loturile mici, și în conformitate cu articolul 60, cele mai multe țări permit o anumită formă de import a medicației pentru uz personal. Este ușor de înțeles de ce pacienții vor căuta un tratament, întrebarea pentru noi, ca fraternitate medicală, este cum răspundem. Siguranța medicamentelor generice - lanțul de aprovizionare deține supremația În ciuda afirmațiilor contrare ale companiilor farmaceutice, multe medicamente sunt foarte ieftine și simplu de produs. Deși există ambele, atât știință cât și artă în furnizarea dozelor de medicament în mod eficient, aceste cunoștințe sunt bine cunoscute și larg dispersate. În mod obișnuit înghit etanol, care aproape sigur nu a fost făcut în conformitate cu cerințele de inspecție complexe ale bunelor practici de fabricație (GMP). O parte din vinul pe care îl beau a fost făcut din struguri zdrobiți cu propriile mele degete, și cu cele ale altora. Este la fel de sigur, steril și perfect precum vinul făcut în fabrică? Probabil că nu, dar se pare că nu îmi face nici un rău mare. În medicină și în farmaceutice cred că ne-am lăsat un pic duși de val. Este rezonabil să se continue a suferi de o boală 20% fatală doar pentru că am 0.1% griji cu privire la proveniența leacului? Punând toate acestea în balanță, cred că nu. Datele din studiile REDEMPTION-1 (16) prezentate la Congresul Internațional al Ficatului (ICL) 2016 al Asociației Europene pentru Studiul Ficatului (EASL) demonstrează în mod clar că siguranța și eficacitatea medicamentelor generice, cel puțin a genericelor utilizate în studiu, sunt echivalente cu medicamentele de marcă și livrează ratele preconizate de +90% de răspuns virusologic susținut (RVS). Doctorii care prescriu și monitorizează pacienții care iau generice se pot simți confortabil din faptul că, precum anterior cu genericele pentru HIV, medicamentele generice HCV dau rezultate clinice robuste. Acest lucru nu sugerează că nu ar trebui să ne preocupe, pentru că o mare atenție este necesară în cazul în care medicamentele generice vor fi utilizate. Atunci când noi, ca medici, scriem numele medicamentelor pe hârtie, depindem în mod normal de o mașină gigantică și bine unsă pentru a livra chimicalele corecte în corpul pacientului nostru. În cazul genericelor, integritatea lanțului de aprovizionare este vitală. La fel cum medicamentele on-line pentru SIDA au devenit un canal de încredere pentru medicația generică HIV, FixHepC.com a ajuns să funcționeze în același rol și oferă un serviciu opțional de 200$ pentru a testa cu RMN o pastilă și a asigura că ea conține ingredientele active dorite în cantitățile corecte. În cazul în care pacientul dvs. are HCV, și se află în posesia unor medicamente generice HCV valide, este evident că se renunță la ecuația risc / beneficiu - cheia este de a se asigura că medicamentele provin din surse de încredere. Astăzi, peste 1000 dintre concetățenii noștri au pierit de o boală pentru care avem puterea de a vindeca. Avem puterea de a „repara” hepatita C. Întrebarea mea pentru voi este, avem puterea voinței? Puterea voinței de a gândi global, dar de a acționa local și să vedem leacul propagat la scară largă? Sau mai degrabă vom proteja orbește drepturile brevetelor în detrimentul vieții pacienților? Genericele funcționează. Haideți să le propagăm și să ștergem hepatita C de pe fața planetei așa cum am făcut cu variola și poliomielita. Confirmări Sprijin financiar: Niciunul. Conflict de interese: Dr. James Freeman asistă pacienții în obținerea accesului la medicamente generice prin intermediul site-ului FixHepC.com și nu a primit nici o plată de la nici un producător API sau companie farmaceutică. Dr. Andrew Hill a primit plăți de consultanță de la ViiV, Gilead, BMS, Cipla si Janssen, care nu au legătură cu acest proiect. Abrevieri BMJ, British Medical Journal; DAA, direct-acting antiviral agents; EASL, European Association for the Study of the Liver; GMP, Good Manufacturing Practice; HBV, hepatitis B virus; HCV, hepatitis C virus; HIV, human immunodeficiency virus; ICL, International Liver Congress; NMR, nuclear magnetic resonance; R&D, research and development; SVR, Sustained Virological Response; TB, tuberculosis; TRIPS, Trade Related Aspects of Intellectual Property Rights; WTO, World Trade Organization. Corespondență Dr James Freeman, GP2U Telehealth, Level 2, 38 Montpelier Retreat, Battery Point, Hobart, Tas. 7004, Australia Tel: +61 1300 472 866; Fax: +61 1800 472 832 e-mail: This email address is being protected from spambots. You need JavaScript enabled to view it. Handling Editor: Francesco Negro Primit pe 23 April 2016; Acceptat 4 May 2016 Referințe a se vedea fisierul PDF // are available in the PDF file
Category: New to Forum
|
|
| 06 Jun 2016 00:42 | |
|---|---|
|
In this post I attach the Romanian translation for the FIXHEPC page "Hepatitis C Genotype Specific Treatments"
In aceasta postare atasez traducerea în limba română pentru pagina FIXHEPC "Tratamentele_specifice_ale_genotipurilor_hepatitei C" 24.August.2015 Tratamentele specifice ale genotipurilor hepatitei C activitatea de traducere a fost efectuată în regim de voluntariat de către un utilizator înregistrat pe platforma fixhepc.com. Deși traducătorul a depus cele mai bune eforturi pentru a furniza o traducere de acuratețe ridicată, acesta nu își poate asuma responsabilitatea asupra ei, în caz de dubii ori în scop de clarificare, textul original, în limba engleză, putând fi consultat la adresa sursă: fixhepc.com/getting-treated/genotype-spe...-hepc-treaments.html 6 Tipuri de hepatită C (Genotipuri) Există 6 genotipuri diferite ale hepatitei C. Genotipurile se referă la natura virusului hepatitei C sau HCV. Deoarece virusul care infestează ficatul poate fi de 6 tipuri diferite, este important să alegi medicația cea mai adecvată pentru genotipul tău. Medicația optimă de tratament (care oferă cea mai mare șansă de vindecare) depinde de genotipul specific pe care o persoană îl are. În timp ce alte tratamente ar putea funcționa bine, există de obicei cea mai bună alegere. Veți găsi rezumate bune, actualizate și fiabile privind cel mai bun tratament pentru genotipul dvs. la oricare dintre:
Rezumatul executiv este (click pe link pentru detalii complete) 1. Pentru genotipul 1, Sofosbuvir + Ledipasvir SAU Sofosbuvir + Daclatasvir +/- Ribavirină (www.hepatitisc.uw.edu/go/treatment-infec...e-1/core-concept/all ) 2. Pentru genotipul 2, Sofosbuvir + Ribavirină SAU Sofosbuvir + Daclatasvir +/- Ribavirină (www.hepatitisc.uw.edu/go/treatment-infec...e-2/core-concept/all ) 3. Pentru genotipul 3, Sofosbuvir + Ribavirină SAU Sofosbuvir + Daclatasvir +/- Ribavirină (www.hepatitisc.uw.edu/go/treatment-infec...e-3/core-concept/all ) 4. Pentru genotipul 4, Sofosbuvir + Ledipasvir SAU Sofosbuvir + Daclatasvir +/- Ribavirină (www.hepatitisc.uw.edu/go/treatment-infec...e-4/core-concept/all ) 5. Pentru genotipul 5, Sofosbuvir + Ledipasvir SAU Sofosbuvir + Daclatasvir (www.hepatitisc.uw.edu/go/treatment-infec...r-6/core-concept/all ) 6. Pentru genotipul 6, Sofosbuvir + Ledipasvir SAU Sofosbuvir + Daclatasvir (www.hepatitisc.uw.edu/go/treatment-infec...r-6/core-concept/all ) Vă recomandăm insistent să consultați medicul despre cea mai bună opțiune de tratament pentru dvs. Circumstanțele dvs. individuale vor sugera regimul optim. Verificați care sunt medicamentele de care aveți nevoie pentru genotipul dvs. de hepatită C Determinarea tratamentului pentru un anumit genotip de hepatită C depinde de alți factori pentru fiecare pacient în parte. Aici sunt o serie de factori medicali pe care medicii îi folosesc pentru a indica tratamentul cel mai optim:
De ce două medicamente pentru tratamentul hepatitei C? Veti observa că, în toate cazurile, sunt necesare cel puțin două medicamente. Motivul pentru aceasta se referă la un fenomen numit moarte logaritmică. Un singur medicament va ucide doar un procentaj din virus. În timp ce acest procentaj ar putea fi într-adevăr mare, să spunem 99,999%, vor exista câțiva supraviețuitori, iar acești supraviețuitori vor fi rezistenți la acest medicament. Asta intră în acțiune cel de-al doilea medicament pentru a-i omorî pe acești supraviețuitori folosind un mecanism diferit față de primul medicament și, astfel, se obține îndepărtarea completă a virusului. Dacă pe de altă parte, virusul nu ar fi complet eliminat (chiar dacă numai 0,001% ar supraviețui), există șanse puternice ca hepatita C să revină atunci când virusul începe din nou să se înmulțească. Al doilea medicament este acolo pentru a asigura că acest lucru nu se întâmplă. Succesul tratamentului hepatitei C Succesul tratamentului este definit ca încărcătură virală zero, și de obicei este măsurată la 12 sau 24 de săptămâni după terminarea tratamentului. Aceasta se numește SVR12 / SVR24 (răspuns virusologic susținut). Unii oameni fac recidivă, care de fapt înseamnă că, deși la analize nu am putut găsi nici un virus, au mai existat câțiva supraviețuitori. În cazul în care un pacient are încă încărcătură virală 0 la un an după tratament, putem fi foarte siguri că acesta e vindecat. Măsurăm prezența virusului hepatitei C prin măsurarea încărcăturii virale. Un tratament de succes cu sofosobuvir și ledipasvir, de exemplu, va scădea încărcătura virală la 0. Asta înseamnă că nu mai există nici un virus detectabil în sânge. Unii pacienți obțin acest rezultat după numai 6 săptămâni din perioada de 12 săptămâni a tratamentului. Este important să nu se oprească tratamentul atunci când încărcătura virală este 0. Tot ar mai putea exista câțiva viruși, sub nivelul de detectare, care s-ar putea manifesta din nou în hepatită C. Pentru a asigura că acest lucru nu se întâmplă, atunci întregul regim de 12 săptămâni de tratament trebuie să fie respectat. Impactul Cirozei asupra Succesului Tratamentului Hepatitei C Cu cât cineva este infectat mai mult timp cu virusul hepatic C, cu atât au loc mai multe daune hepatice. Aceste daune se repară cu țesut cicatricial fibros și provoacă ciroza. Ciroza poate duce la insuficiență hepatică și deces și crește riscul de a dezvolta cancer la ficat. Măsurăm ciroza, folosind o mașină de Fibroscan și de obicei vorbim despre ea în termenii unei scale "F", în care F0 înseamnă bine și F4 indică prezența cirozei. In termeni simpli, ciroza scade ratele de vindecare de la aproximativ 95% la aproximativ 85%, așa că este mai ușor să tratezi un pacient înainte de a se intampla acest lucru. De asemenea poaate fi necesar să se crească durata tratamentului de la 12 săptămâni la 24 de săptămâni. Aceasta are legătură cu dificultatea medicamentului de a intra în țesutul fibros care are o aprovizionare relativ slabă cu sânge. Cu ribavirină sau fără ribavirină - aceasta este întrebarea Știm că fiecare medicament va oferi o „moarte logaritmică” (log-kill) și se poate observa că în cazul HIV (de asemenea un virus ARN), că un medicament este bun, două sunt și mai bune, iar trei pot fi iarăși mai bune. A se vedea, ART si HAART. În data de 25 aprilie 2015 la Conferința Internațională a Ficatului a fost prezentat un document: www.eurekalert.org/pub_releases/2015-04/eaft-sce042415.php care sugerează că adăugarea de Ribavirină la Sofosbuvir și Daclatasvir s-ar putea dovedi a fi benefică, totuși din cauza mărimii mici „n” a eșantionului, marja de eroare cu privire la aceste rezultate oarecum încurajatoare este mare (10%). Ribavirina nu este la fel de toxică precum PEG interferon, dar are substanțial mai multe efecte secundare decât Sofosbuvir, Daclatasvir și Ledipasvir.
Category: New to Forum
|
|
| 25 May 2016 08:35 | |
|---|---|
|
With any new drug many impacts are unknown.
If you search for "sofosbuvir semen" on Google you will only find 2 results. Sofosbuvir was previously known as PSI-7977 and GSI-7977 so you should also search for pharmasset psi-7977 semen gilead gsi-7977 semen The last search yields this result: www.natap.org/2014/EASL/nejmoa1316366_protocol.pdf however the excretion in semen refers to Ribavirin. Anyway in the absence of documentation saying it's not in semen you would be safest to refrain from trying to have children during treatment. The logic for how long to wait after treatment see: fixhepc.com/forum/experts-corner/872-how...etting-pregnant.html
Category: FixHepC Admin
|
|