
It's come to my attention that some people on the Internet are "bad-mouthing" Maviret (Mavyret) and suggesting it's the worst option on the market and that you need Sofosbuvir. Anyone stating this does not, as they say, know their ass from their elbow - this drug is awesome where awesome means great cure rates, short duration of treatment, and minimal side effects. While there is no doubt Sofosbuvir based regimens are also great there are very few patients for whom they might be superior.
Let's start with the spelling. Is it Maviret or Mavyret? The answer is it's both! The combination of Pibrentasvir and Glecaprevir from Abbive goes by both names, depending on the market. Let's call it G/P for short, after all, that's what most doctors call it.
Common things happen commonly
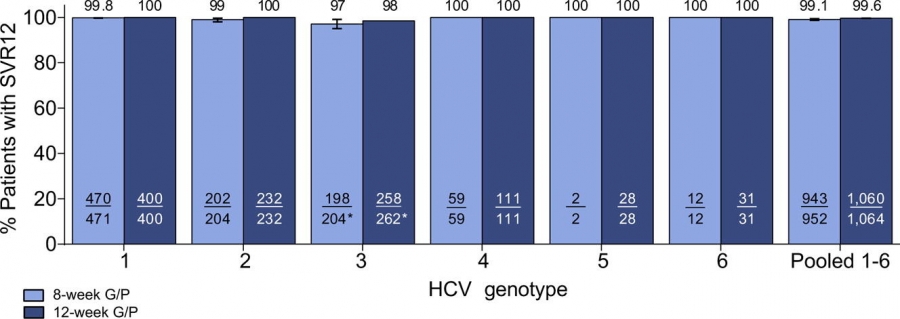
Now let's have a look at the profile that fits the vast majority of patients - treatment naive, low fibrosis. Here is a link to the seminal study in the Journal of Hepatology: https://www.journal-of-hepatology.eu/article/S0168-8278(18)30165-X/fulltext looking at the results for G/P

And I could probably stop here because let's face it, that's pretty amazing. Did I mention this G/P combination is awesome?
Now, by way of comparison let's pull out Gilead's latest and greatest 2 drug combination - Epclusa - aka Sofosbuvir + Velpatasvir. How does that perform in the most common case?
Here it is: http://www.natap.org/2016/DDW/DDW_13.htm and looking at the SVR12 results we see:
Hmm, that looks similar but, dare I say, a little worse. Not quite as good in the most common GT1 patients, or the next most common GT3 patients, or the next most common GT2 patients. Now don't get me wrong, it's far from shabby and there is, in fact, no statistical difference but it does rather put to rest the notion that G/P is inferior.
Patients with cirrhosis
Ok, so let's dig into the hard cases -patients with cirrhosis. For G/P in GT1,2,4,5,6 it looks like this http://www.natap.org/2018/AASLD/AASLD_17.htm
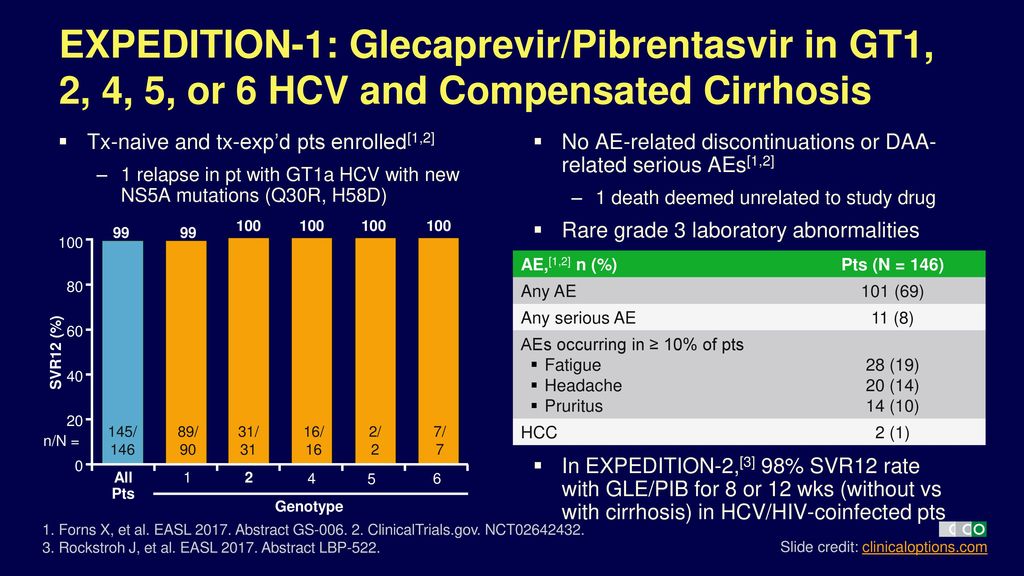
There's not a lot to say about that other than it's not what we usually expect with significantly reduced SVR12 in patients with cirrhosis.
GT3 Cirrhotic Patients
And, finally, let's get into the really hard basket - GT3 patients with cirrhosis +/- treatment experience
For G/P in GT3 with cirrhosis +/- treatment experience it looks like this: http://www.natap.org/2017/HCV/092217_01.htm
Does a sofosbuvir based regimen have any advantages over G/P?
So do Sofosbuvir based regimens have any advantages over G/P? Yes, there are several special use cases for it. For example, G/P can't be given to people with decompensated cirrhosis, whereas Sofosbuvir-based regimens can: http://www.natap.org/2015/AASLD/AASLD_64.htm and they work pretty well:
There are a few other circumstances where you would prefer a sofosbuvir-based regimen but these are rare and relate to treatment experience and retreatment and in this case you should be consulting an expert for advice, not the Internet.
Conclusions
Personally, I'd be happy to have either G/P or a Sofosbuvir based regimen. I would not be at all worried about being prescribed G/P, in fact I might well secretly be pleased, not only because of the short duration and favourable side effect profile but because if you add Sofosbuvir to G/P you have the most potent 3 drug combination for HCV that is available, ideal for retreatment, but that, as they say, is a story for another day.

{kind=link}