
Home › Forums › Main Forum › Experts Corner › IL28 Explained
- This topic has 4 replies, 3 voices, and was last updated 10 years, 5 months ago by
 Gaj.
Gaj.
-
AuthorPosts
-
28 January 2016 at 8:50 am #10638
IL28 is a gene.
Like most genes you get 1 from mum, and 1 from dad.
You can get either a “C” or a “T” IL28 gene from each of your parents.
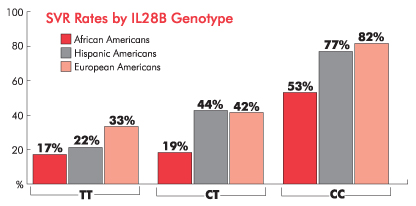
In the days of interferon having “CC” ie 2 copies of the “C” IL28 gene improved your chances of SVR. Two copies of the “T” ie “TT” predicted you would probably fail. As you might expect “CT” or “TC” ie one “C” and one “T” from your parents put you in the middle.
With DAAs it’s not really important because TT, CT and CC people all do well. It’s probably still a little advantageous to have “CC” but there is little point in testing for this these days, and after all, there is nothing you can do about it.
YMMV
28 January 2016 at 10:59 am #10646I was wondering about this the other day when you posted the new Decision Support Tool.
i.e. For genotypes 2/4/5/6 is there any advantage when making a decision on treatment for the new Australian guidelines that recommend Peg/Riba with Sofosbuvir? Eg “if the patient has TT and maybe CT then follow EASL guidelines and prescribe Sof/Dac”
Or would using Sof with the Peg/Riba negate any advantage there?
G3a since ’78 – Dx ’12 – F4 (2xHCC)
24wk Tx – PEG/Riba/Dac 2013 relapsed
24wk Tx – Generic Sof/Dac/Riba 2015/16 relapsed
16wk Tx – 12/01/17 -> 03/05/17 NS3/NS5a + Generic Sof
SVR7 – 22/06/17 UND
SRV12 – 27/07/17 UND
SVR24 – 26/10/17 UND
 28 January 2016 at 11:49 am #10650
28 January 2016 at 11:49 am #10650Ah yes and after the tx failed me and popped me into hospital and so on they did my Il28 and I was CT
Hmmmmm
Thanks to the FixHepC people for my Sof/Led it’s changed my life and I haven’t even had my first bloods done yet. You have given this liver clinic bench warmer hope and a brighter future29 January 2016 at 1:03 pm #10717The AUS rules are the expected PBS restrictions. The PEG/RIBA free ones are what I would want for my mum.
YMMV
29 January 2016 at 2:34 pm #10729Hmmm, on further reflection peg/riba is sub optimum for everyone regardless of their genes.

While it’s reasonably cost achievable to help our mums the best scenario is that PBS doesn’t end up discriminating against 9% of HCV infected people to save a few bucks.
Anyone know when the final rules get announced?
G3a since ’78 – Dx ’12 – F4 (2xHCC)
24wk Tx – PEG/Riba/Dac 2013 relapsed
24wk Tx – Generic Sof/Dac/Riba 2015/16 relapsed
16wk Tx – 12/01/17 -> 03/05/17 NS3/NS5a + Generic Sof
SVR7 – 22/06/17 UND
SRV12 – 27/07/17 UND
SVR24 – 26/10/17 UND
-
AuthorPosts
- You must be logged in to reply to this topic.