| Welcome, Guest |
TOPIC:
Text of email conversation with Mrs Debbie Romesburg 7 years 2 months ago #24288
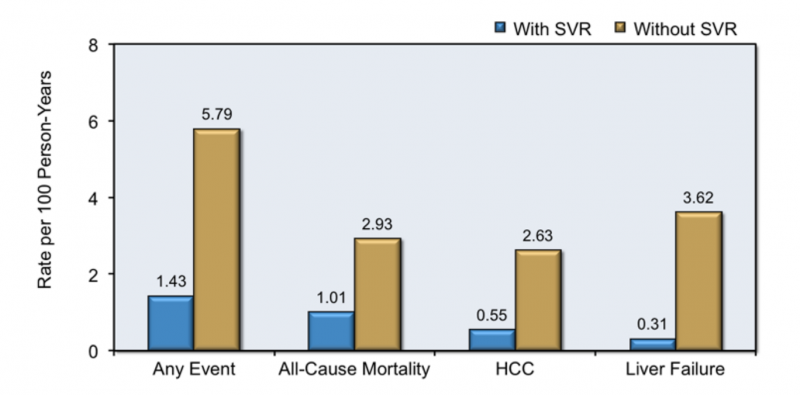
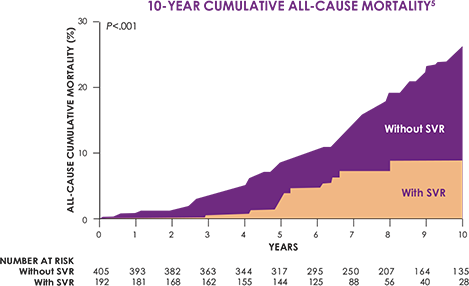
Hi Debbie, Sorry to hear about your husband but the reality is that in a patient population in the age range 45-65 heart attacks happen at significant rates with or without treatment. Here is part of an email from this morning: Good Afternoon Just to let you know that following my Coronary problems in January, I am lucky enough to have recovered very well and feel generally in good health. My Cardiologist tells me that he feels that I am now strong enough to start the medication. There is a however a possibility that I will require a further stent over the coming months. I have started the first 3 month Sofosbuvir/Velpatasvir course today. Now obviously drugs this patient was not taking could not have caused their heart attack, but that heart attack still happened. It sounds to me as though you think you have found a scandal/cover up. I really don't think you have, and I'm one of the better-informed doctors in the world. I say that because I personally have well over 1000 patients who have taken DAAs, have collated the results, and have no connections to Big Pharma. There is nothing much unexpected to be found. Most patients do well, a few don't. Far more patients do well than with the older treatments. In short, these drugs are much much safer than the disease they are treating and much safer than what we used to use. That is a good as it gets in medicine. Perfect, certainly not. Good enough, absolutely. Would I treat my mother with them? Without hesitation. Before wasting a large quantity of time and emotional energy on your campaign I suggest you acquaint yourself with statistics like these which document cardiovascular disease in the general population: www.heart.org/idc/groups/heart-public/@w...dable/ucm_449846.pdf In medicine we say common things happen commonly. Heart attacks are common so they happen commonly. You can only implicate a drug if they happen more commonly than expected. Even if that was the case, and as far as I can see it's not, then you have to weigh up the risk/benefit. With Vioxx for arthritis, the increased rates of heart attacks were significant not simply because they happened but far more importantly because the disease being treated was mild, and there were/are better alternatives. If Vioxx had been treating cancer it would almost certainly still be on the market because we, as in the medical profession would have gone, ok, so a few extra patients have heart attacks but the risk/benefit still stacks up. To be frank I'm actually surprised we don't see more on treatment heart attacks than we do. With interferon, you were 3 times less likely to die in any given year if you were cured. That 2.93% annual mortality rate is what you get if you don't treat patients. The 1.01% is what you see if you do and they SVR. Hep C kills people. By year 10 it has killed nearly 30% of the people that have it. It kills a lot less at SVR, and by 10 years post treatment, the mortality rate has stabilised. It is still higher than the general population, but much lower than the still infected population. Patients who have Hep C are also observed to have much higher than expected rates of a range of non-liver related diseases. This has nothing to do with treatment, it's where they are at baseline. www.ncbi.nlm.nih.gov/pmc/articles/PMC4735500/
All those risks stay unchanged in the absence of treatment. It would be sad to see patients scared of taking treatment because of something that looks like a ~1% serious side effect risk profile and continue to suffer from a disease with a very significant mortality rate. This totally ignores the quality of life issues, and the vast majority of patients are much better after treatment. You will find an analysis of an FOI request to the FDA's FEARS database here: fixhepc.com/forum/experts-corner/786-off...-effect-reports.html I would strongly suggest you make a new FOI request and then do a statistical analysis of it. If what you believe is true, then it will show up there, unless you wish to believe that every physician in the USA is corrupt and not reporting side effects they are observing in their personal patients. While you are there it would also be useful to get a set of data for, say an HIV/Hep B drug like Tenofovir to provide a reasonable comparator. From time to time s**t happens for every single drug we have available. Even water, oxygen and carbon dioxide can be fatal. Nothing is 100% safe, so everything needs to be assessed on a risk/benefit basis. The best outcome I can see from your quest is to scare a whole lot of people out of getting treatment who will then, as a direct result, suffer/die of a disease they could have been cured from. That is not something I would want to be remembered for, nor something I can support or assist you with. YMMV | |
{kind=link}
{kind=link}
Text of email conversation with Mrs Debbie Romesburg 7 years 2 months ago #24290
| Amen brother James, amen. Contracted HCV 1980's Geno Type 1a F3 ( doc says once treated I'll be F2 maybe F1) Meds shipped 6/17/2016 arrived early 7/2016 Viral count - 3,471,080 4 week quantitative bloods: August 17, 2016. I have been diagnosed as <15 (told undetected) 8 week quantitative bloods: September 14th. I have been diagnosed as <15 (told undetected) 11 week PCR RNA Qualitative bloods: September 26th 2016 - Undetected December 19th 2016: Cured! Viral count: zero!!! 2018 viral count: still zero! Cured! | |
Text of email conversation with Mrs Debbie Romesburg 7 years 2 months ago #24291
| Hi Debbie, just my bit ..... "I have lost 10 friends from the USA treatment and 12 develop Cancers. I have numerous friends complaining of RA and fibermyalga. They are complaining of Teeth problems, stomach issues. Bone issues". This does have a familiar ring to it when I think back about many of the comments that have been made about Interferon (plus/minus Ribavirin) treatment. My personal dislike was/is Ribavirin, which I regarded when mixed with Interferon as just an alternative to arsenic. This time around, with re-treatment on DAA's and having had a taste of life HCV free, I find Ribavirin is a necessary evil to get a cure - although it made me feel like sh*t. Medically, I am assured that the HCV led me to have a HCC. The HCV, I say, caused me to live a lesser life because of the fatigue. I have some good reason to believe this as the fatigue went during treatment with DAA's, and came back when the virus returned. Second time around with re-treatment, it is harder to define as Ribavirin tends to knock me around; but post treatment and at this time HCV free, I am slowly feeling better. Just a bit of a ramble but I think that quality of life (free of HCV) needs to be 'factored in' to any decision to use DAA's. For me, treatment with them wins hands down all the time. Yours Jeff. GT3a 1990 Failed Inter 1998, comb in 2000. HCC 2012 Started 24/52 Sof/Dac 27th October 2015. 1. Bloods 2 October 2015: AST - 165 (20-40), ALT - 265 (5-40), GGT 189 (5-50) 2, Bloods 20 November 2015: ALT etc normal; VL 19 3. Bloods 8 January 2016: AST - 40, ALT - 59, GGT 48 VL RNA UND 4. EOT 12 April 2016 - blood tests: all is well, CT scan: okay 5. AFP 11 June 2016: 4 ref< 11 6. VL July 2016: DET 7. Oct16 start treat - June17 UND 8. Jun 18, lfts okay, platelets a bit low. | |