| Welcome, Guest |
TOPIC:
Baby Boomers 8 years 2 months ago #14855
| Many people believe that if you have hepatitis C then it automatically means that you fall into one of the four following categories (a) you are/were an intravenous drug user (b) you got it from a blood transfusion (c) you got it from violent unprotected sex (d) you are a liar Here is a story about "baby-boomers" and hepatitis C: www.theglobeandmail.com/news/british-col...ind/article29488842/ Here is the original article in the Lancet: www.thelancet.com/journals/laninf/articl...6%2900124-9/abstract I remember when I was a kid at junior school (late 1960s), the whole class was lined up to go to the clinic just next to the school for BCG jabs. What I do not remember is whether in those days the nurse used a disposable syringe or not because the nurse always turned out heads away before the jab... And anyway, this is not the kind of thing a 10-year-old kid would think to ask Does anyone know when disposable one-shot syringes were first used by the NHS or elsewhere? Please note, I am not trying to blame the NHS for anything here. The hepatitis C virus was only discovered in 1989, and so anyone (or any institution) who re-used syringes before that date should not be blamed for something that was not medically known at the time. But if there really is a proven link between vaccinations and the spread of the virus, it could help to remove a lot of the stigma that exists today... Diagnosed Jan 2015: GT3, A0+F0/F1. Fatigue + Brain-Fog. Started Sof+Dac from fixHepC 10-Nov-2015. NO sides. Pre-Tx: AST 82, ALT 133, Viral Load 1 900 000. Week4: AST 47, ALT 58. VL < 15 (unquantifiable). Week12 (EOT): AST 30, ALT 26, VL UND Week16 (EOT+4): AST 32, ALT 28, GGT 24, VL UND Week28 (EOT+16): AST 26, ALT 22, GGT 24, VL UND Ever grateful to Dr James. Relapsed somewhere after all that... Bummer! Jan 2018: VL 63 000 (still GT3). | |
Baby Boomers 8 years 2 months ago #14867
| Hi Vororo, The fully disposable syringe was invented by Colin Murdoch, a New Zealand pharmacist, in the year I was born (1956). Obviously it took a while after that to come into common let alone universal use. I have early childhood memories of GP inoculations being given by syringes that were shiny and "clinked" when returned to the little metal tray they used and just the fact that they put it back on the tray would indicate it probably wasn't disposable. This occurred prior to migrating from UK to Aust so very early sixties when I was maybe 3-6 yr old? Having said that and while it doesn't matter much anyway, I can state that I'm a gentle soul and with conviction that it isn't possible that I contracted HCV from method (b), which leaves (a) unless (d) applies. There are also some interesting studies of how it appears to have spread outwards into the community from Glasgow hospitals post WW2. So while I suspect us BBs have caused some interesting patterns and swirls in the dissemination of HCV, the research does seem to indicate that the greatest spread has occurred due to knowledge/technology/military issues rather than allegedly "moral" ones. G3a since '78 - Dx '12 - F4 (2xHCC) 24wk Tx - PEG/Riba/Dac 2013 relapsed 24wk Tx - Generic Sof/Dac/Riba 2015/16 relapsed 16wk Tx - 12/01/17 -> 03/05/17 NS3/NS5a + Generic Sof SVR7 - 22/06/17 UND SRV12 - 27/07/17 UND SVR24 - 26/10/17 UND The following user(s) said Thank You: Vororo, Tina-Hill-facebook | |
Baby Boomers 8 years 2 months ago #14875
| Yeah Gaj and V, A lot of blood flowing during the first half of the 20th century all over the world. Given the unsanitary conditions, both on the battlefield and off, its no surprise that a blood borne disease went "viral". Add Korea and Vietnam, factor in the mass smallpox and polio vaccinations and you have a perfect setting for an epidemic. This email address is being protected from spambots. You need JavaScript enabled to view it. forums.delphiforums.com/generichcvtx G 1a F-1 Started tx 10/23/15 (Meso sof & led) ALT 48 AST 28 v/l 1.6 mil 11/17/15 4 wk lab ALT 17 AST 16 <15 11/18/15 Started Harvoni 12/16/15 8 wk lab ALT: 15 AST: 13 V/l UND 1/14/16 Fin. Tx 7/07/16 UND SVR 24 The following user(s) said Thank You: Gaj | |
Baby Boomers 8 years 2 months ago #14877
Good deduction there Mike, so how did the various genotypes come about? Just asking cause that area always confuses me. G1a dx'd in 1992, Biopsy F2 VL 8mill +. Tried tx with Interferon/Riba, back in 2008 didn't last long it felt horribly ugly!! I stopped tx, after 5 weeks!! Started tx 6/1/16 with Harvoni. 12 Month Labs= UND | |
{kind=link}
Baby Boomers 8 years 2 months ago #14885
Yeah, no doubt technology and bloody wars contributed a lot to the spread. But the fact that there are 6 genotypes or more must mean that the virus has been in the human population for a very long time. Until modern medicine came along, human life expectancy was only about 30 years. So back in ancient times the chances are pretty high that anyone with the virus would die of something else long before it would cause any problems... en.wikipedia.org/wiki/Life_expectancy Diagnosed Jan 2015: GT3, A0+F0/F1. Fatigue + Brain-Fog. Started Sof+Dac from fixHepC 10-Nov-2015. NO sides. Pre-Tx: AST 82, ALT 133, Viral Load 1 900 000. Week4: AST 47, ALT 58. VL < 15 (unquantifiable). Week12 (EOT): AST 30, ALT 26, VL UND Week16 (EOT+4): AST 32, ALT 28, GGT 24, VL UND Week28 (EOT+16): AST 26, ALT 22, GGT 24, VL UND Ever grateful to Dr James. Relapsed somewhere after all that... Bummer! Jan 2018: VL 63 000 (still GT3). | |
Baby Boomers 8 years 2 months ago #14888
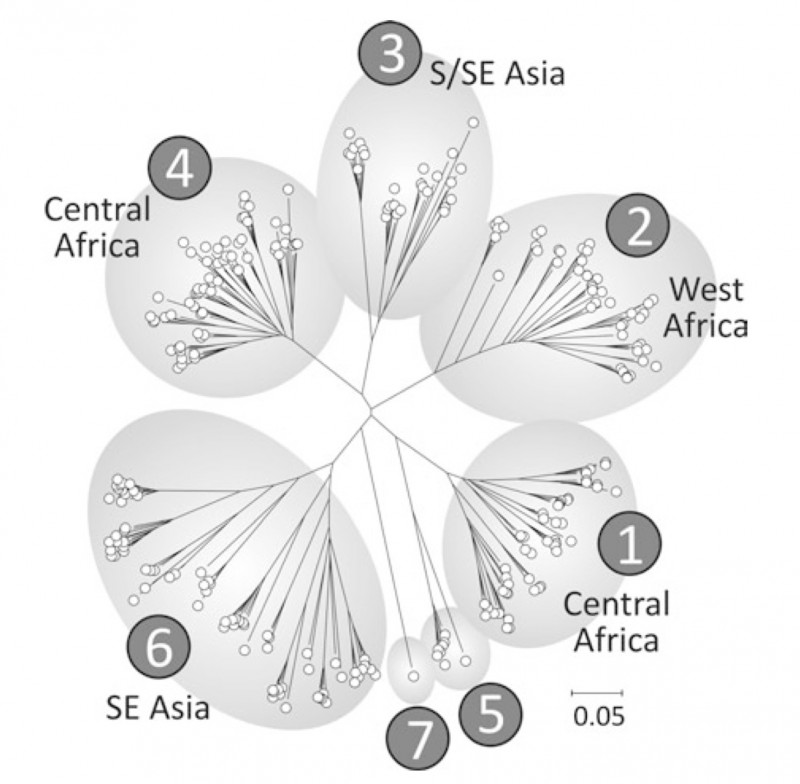
Okay, so I'll try and give this a go from an evolutionary genetics perspective: As Vororo says HCV has been around for a long time. Basically we probably started out with either one (or possibly a very few) strain of HCV which crossed the barrier from some other host into the human population. Viruses don't breed though so they basically replicate themselves with each generation being the same as the previous one. The exception to this rule is when they mutate into something different but in almost all cases the mutation will be weaker than the original strain and won't be as successful at replicating so will die out or be killed off by its hosts immune system ending that new strain before it has a chance to spread into other hosts. But very, very occasionally the mutation will be successful. It will be good at replicating itself accurately and may have an advantage over the original in how it manages to evade our immune system. So it will continue to thrive and may get lucky enough to spread into other peoples bloodstreams. If it does that often enough then that strain will likely continue into the future as a new genotype or subtype. Now, the chances of genotype 1b mutating into 3a are so infinitesimally small that basically "it ain't gonna happen!". But what will happen is that 1a will become 1ax or 1ay or if it is different enough it will create a new genotype, say GT8 or whatever we decide to call it. Here you have to remember that because HCV is only spread by blood to blood contact it has a linear transmission path so in ancient times you would find that all the people infected in an area would have the same or similar genotypes/subtypes. Until you throw in population movement, migration and now modern jet travel, etc. then we start to get a mix of types across the world. Below is a great picture that shows the main genotypes by their place of origin/greatest commonality. The interesting thing to note is that while there are 7 main genotypes there are many, many more subtypes. Some of these subtypes have or will die out, other new ones will be created. This is a bit like human genetics in that there are people who are blue eyed, and of these some will have blonde hair. So we have blue eyed/blondes but even within this grouping there will be some with straight hair, some with wavy hair, some with curly hair and some with frizzy hair. Each of the Geno-subtypes is a bit like that. But to keep things simple and because all the genotype 1a subtypes are very similar, we just say they are 1a. (Or blue eyed/blondes). Hopefully all that makes sense as a very simplistic G3a since '78 - Dx '12 - F4 (2xHCC) 24wk Tx - PEG/Riba/Dac 2013 relapsed 24wk Tx - Generic Sof/Dac/Riba 2015/16 relapsed 16wk Tx - 12/01/17 -> 03/05/17 NS3/NS5a + Generic Sof SVR7 - 22/06/17 UND SRV12 - 27/07/17 UND SVR24 - 26/10/17 UND | |
{kind=link}
Baby Boomers 8 years 2 months ago #14890
| 1970s dentists (and in fact dentists 2015) I was never taught to avoid the blood of others. We even used to do that pin-prick blood brothers / sisters thing way back when. I think medical procedures especially in the 60s/70s have helped the virus spread, no doubt about that in my mind GT1a Dec14 F2/8.7 VL 900000-2.5M Jan16 Hepcivir-L MonkMed/Redemption Baseline: VL 913575 Alt 76 Platelets low Wk2 VL1157 Alt 23 DET Wk 8 VL 32 Alt19 'In the slow lane' June16 Fibro 5.7 F0/1 LIF 1.5 Wk 11 VL<12 Alt 13 Det/Unq Extending tx 12 wks Mylan Sofo/Dac MonkMed Wk 14 VL <12 Det/Unq Wk 16 VL UNDETECTED Wk 22 + 4 Wks Sunprevir FixHepC Wk 24 UNDETECTED Alt 13 Wk 12 post tx SVR12 Wk 26 SVR24 Thank-you Tim, Dr Debasis @ MonkMed & Dr Freeman @ Fix HepC |
Baby Boomers 8 years 2 months ago #14892
| Thanks Gaj for the nice explanation and graphic. Thanks Londongirl, also. There is probably a good evolutionary reason for our fear of dentists But the thing that still bothers me is how it was transmitted before battle-axes, syringes, and dentists were invented? Current medical opinion says it was not by insect bites, even though insects are the main vector for the other flaviviruses (en.wikipedia.org/wiki/Flaviviridae). ... Dog-bites? Diagnosed Jan 2015: GT3, A0+F0/F1. Fatigue + Brain-Fog. Started Sof+Dac from fixHepC 10-Nov-2015. NO sides. Pre-Tx: AST 82, ALT 133, Viral Load 1 900 000. Week4: AST 47, ALT 58. VL < 15 (unquantifiable). Week12 (EOT): AST 30, ALT 26, VL UND Week16 (EOT+4): AST 32, ALT 28, GGT 24, VL UND Week28 (EOT+16): AST 26, ALT 22, GGT 24, VL UND Ever grateful to Dr James. Relapsed somewhere after all that... Bummer! Jan 2018: VL 63 000 (still GT3). | |
Baby Boomers 8 years 2 months ago #14895
| Big birthday coming up for Gaj. Hope you are going to have a big festival of Gaj (I did last year and it was epic) Genotype 1a Diagnosed in 2004, had HCV for all my adult life. Until 2016!!!! Harvoni treatment, started 19 March 2016 4 week results Bilirubin 12 down from 14 pre treatment, Gamma 25 down from 52, ALT 19 down from 63, AST 19 down from 47, VL <15 down from a lazy 6 million or so EOT Results Bilirubin 10, GGT 18, ALT 19, AST 21, VL UND 12 Weeks post EOT Bilirubin 11, GGT 16, ALT 22, AST 20, VL UND Cured baby The following user(s) said Thank You: Gaj | |
Baby Boomers 8 years 2 months ago #14896
Very good analogy of how things came about. So if its been around since ancient times, how has that been determined? Have mummys been found to have HepC? G1a dx'd in 1992, Biopsy F2 VL 8mill +. Tried tx with Interferon/Riba, back in 2008 didn't last long it felt horribly ugly!! I stopped tx, after 5 weeks!! Started tx 6/1/16 with Harvoni. 12 Month Labs= UND | |
{kind=link}
Baby Boomers 8 years 2 months ago #14909
Probably that or horses is how it got into the human population in the first place but dogs haven't been domesticated long enough for it to have been a common vector within our species. On the other hand, injuries during hunting or just the scratches and cuts of general living plus huddling together for warmth at night pre-fire? Scarification? And all baby boomers will have seen the opening sequence to 2001: A Space Odyssey so will realise that even before battle axes, blood stuck to the nearest available branch/club.
I don't believe so. Basically it's figured it out from the RNA sequence evidence that was used to draw up the graphic I posted. If you know what Genotypes/subtypes are around now and their relationship to each other genetically plus how often the virus successfully mutates on average, you can work backwards to determine at what points the branches in the genetic tree occurred and how long it has been around. G3a since '78 - Dx '12 - F4 (2xHCC) 24wk Tx - PEG/Riba/Dac 2013 relapsed 24wk Tx - Generic Sof/Dac/Riba 2015/16 relapsed 16wk Tx - 12/01/17 -> 03/05/17 NS3/NS5a + Generic Sof SVR7 - 22/06/17 UND SRV12 - 27/07/17 UND SVR24 - 26/10/17 UND | |
Baby Boomers 8 years 2 months ago #14910
| Thanks beaches, this year the festivities fall just after EOT so there will be much (low carb) feasting but rather limited sacraments. G3a since '78 - Dx '12 - F4 (2xHCC) 24wk Tx - PEG/Riba/Dac 2013 relapsed 24wk Tx - Generic Sof/Dac/Riba 2015/16 relapsed 16wk Tx - 12/01/17 -> 03/05/17 NS3/NS5a + Generic Sof SVR7 - 22/06/17 UND SRV12 - 27/07/17 UND SVR24 - 26/10/17 UND | |
Baby Boomers 8 years 2 months ago #14917
| I understand HCV has been around a long time. Also, that different genotypes exist and are prevalent in different geographic locations. The point I was trying to make was the world has gotten much smaller. Huge, bloody wars between groups of people halfway around the worlds from each other came along with the second industrial revolution. So, there was a lot of opportunity for exposure to genotypes not common in certain areas, like between the Japanese and the Allied forces fighting in the Pacific. Vietnam, Korea...a lot of blood... I teach U.S. history. I could fill a whole year talking about nothing but wars. We just don't seem to be content living in peace. m This email address is being protected from spambots. You need JavaScript enabled to view it. forums.delphiforums.com/generichcvtx G 1a F-1 Started tx 10/23/15 (Meso sof & led) ALT 48 AST 28 v/l 1.6 mil 11/17/15 4 wk lab ALT 17 AST 16 <15 11/18/15 Started Harvoni 12/16/15 8 wk lab ALT: 15 AST: 13 V/l UND 1/14/16 Fin. Tx 7/07/16 UND SVR 24 | |
Baby Boomers 8 years 2 months ago #14964
Yes V, I remember lining up for TB vaccinations at school. Australia in the 1960s. As for stigma, I had an ugly experience yesterday at the chemist. I was there with my elderly mother who was filling a script. It’s a busy pharmacy adjacent to a busy bulk-billing (ie free) medical clinic on the border of Queensland and NSW. While waiting I heard the senior pharmacist complaining to another elderly customer about the new Hep C medications. How they cost her $22,000 for each 12 week treatment. How she refuses to stock them. How ‘they’ don’t deserve to get medication on the PBS when ‘they’ are responsible for getting Hep C in the first place. I was dumbstruck. I didn’t expect to hear such malicious misinformation from a health professional, or in such a public way. So I took her aside and let her know I strongly disagreed with her views. How for a start not everyone with Hep C got it from using drugs (the faces of Lynne and Tina helped me along here, as I tried to shove my own guilt aside). How the new meds are saving lives. Her response was about how much her husband’s cancer and chemo treatment are costing, while ‘those drug addicts at Mirikai’ (a Gold Coast rehab) pay only $6.20. I didn’t think to say sorry about your husband. Maybe that would have softened this stressed out, angry and intolerant person. Or not... Instead I pointed out that her attitude is discriminatory, and exited with ‘someone in your position should know better than to mouth off like that’. My blood was boiling. Do I take this further? Name and shame? Complain to the Health Care Complaints Commission? Or let it go as another sad example of human ignorance? To remove the stigma of Hep C, perhaps we need to remove Hep C. NSW Australia. Genotype 1b 30+ years, F0-F1, VL 91,000 Feb 2015 (740,000 in 2010), Tx naive. Ordered Sof/Dac from Buyers Club 21 Sept, received 14 Oct. Virus UNDETECTED at 3 weeks AND 12 weeks (EOT) AND SVR4 AND SVR12 AND SVR24. A thousand thankyous to Dr James and the amazing FixHepC team. | |