
Home › Forums › Main Forum › FixHepC Admin › 4 week blood test advice needed.
- This topic has 9 replies, 3 voices, and was last updated 7 years, 8 months ago by
 Dr James.
Dr James.
-
AuthorPosts
-
16 July 2018 at 7:45 am #28335
Hi , needing advice.
I am on Epclusa 12 week treatment. Just finished week 1.
I am due for my 4 week check soon but will be traveling at that time. Week 6 is the soonest I can get checked. My question is: Is it essential for a 4 week check or is 6 weeks ok too? Will this make any big difference?
thanks
B.16 July 2018 at 8:47 am #28336Hello hovis,
In terms of the treatment testing makes no difference to the outcome.
In terms of predicting if longer than 12 weeks would be beneficial, the only solid data relates to being undetected/detected at 4 weeks. The ~ 20% of people still detected at 4 weeks are 2-2.5x as likely to fail treatment so, if a patient falls into this group it is worth considering extending the treatment past12 weeks.
If you test at 6 weeks you will almost certainly be undetected but that’s all it tells us. If it was still detected that would be a “better do something” kind of a moment, but it’s highly unlikely that this will be the case.
YMMV
16 July 2018 at 9:23 am #28337Hi James, ok thanks that clarifies things for me and in the unlikely event that I have one of those “better do something” moments , you will hear from me.
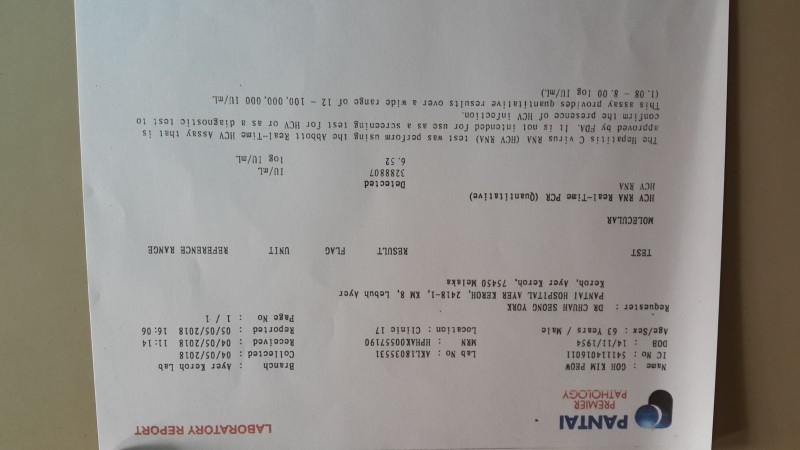
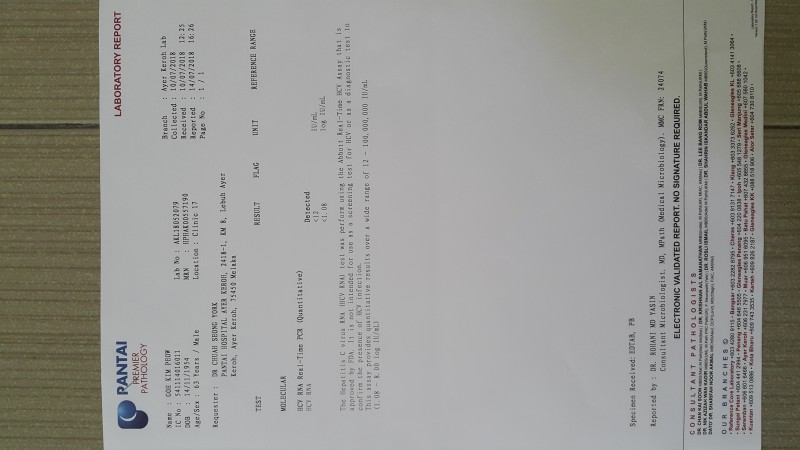
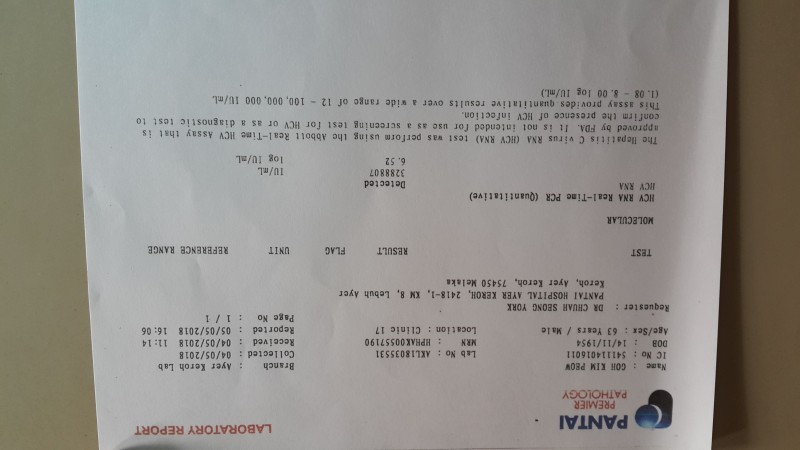
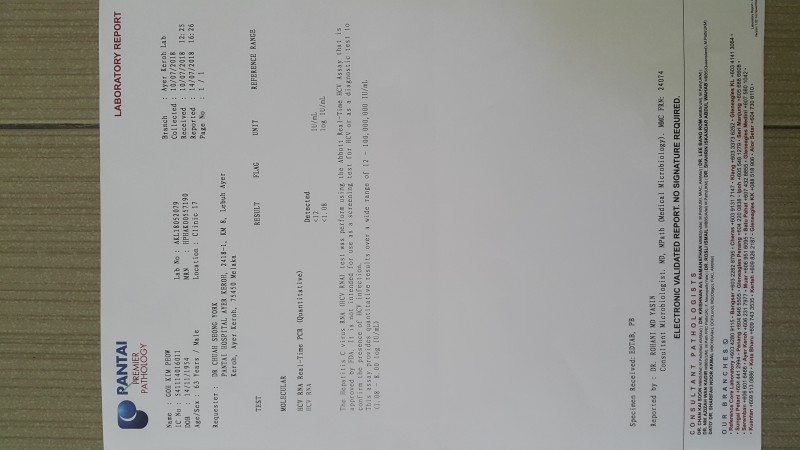
thanks,18 July 2018 at 7:15 am #28341If the weeks 4 viral load result is <12IU/ml but not mention undetected. This means still got small amount of virus?
If refer to this assay provides quantitative results over a wide range of 12~100,000,000 IU/ml. Is it <12 IU/ml is means virus undetected? I'm genotypes 3 n decompensated liver cirrhosis. Do I need to extend my treatment if first weeks 4 viral load result is <12IU/ml?Attachments:18 July 2018 at 7:18 am #28344Carolwinnie wrote:If the weeks 4 viral load result is <12IU/ml but not mention undetected. This means still got small amount of virus?
If refer to this assay provides quantitative results over a wide range of 12~100,000,000 IU/ml. Is it <12 IU/ml is means virus undetected? I'm genotypes 3 n decompensated liver cirrhosis. Do I need to extend my treatment if first weeks 4 viral load result is <12IU/ml?Attachments:18 July 2018 at 11:31 am #28345Hello Carolwinnie,
Yes, the second test says <12 but still detected (so we can still see a trace).
The <12 test is more sensitive than the <15 and <25 and <30 tests so is the "least worrying" of the
YMMV
18 July 2018 at 12:22 pm #28351Thanks for the prompt reply Dr. James.
Actually is my father has HCV.
Patient age : 63
Genotype 3 with decompensated liver cirrhosis & treatment naive.
The medication my father taking is Myhep all (sofosbuvir+velpatasvir)+ribavirin for 12 weeks.
Our doctor did not recommend us to do the fibroscan.
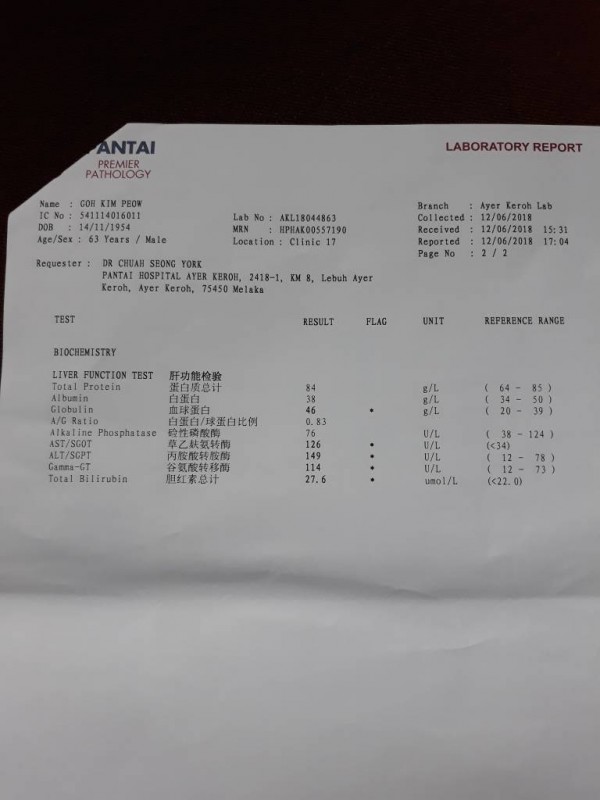
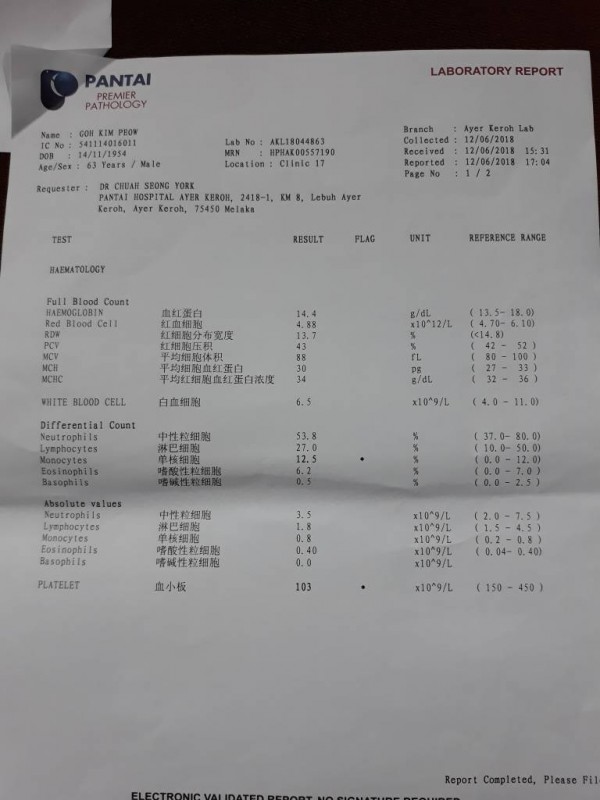
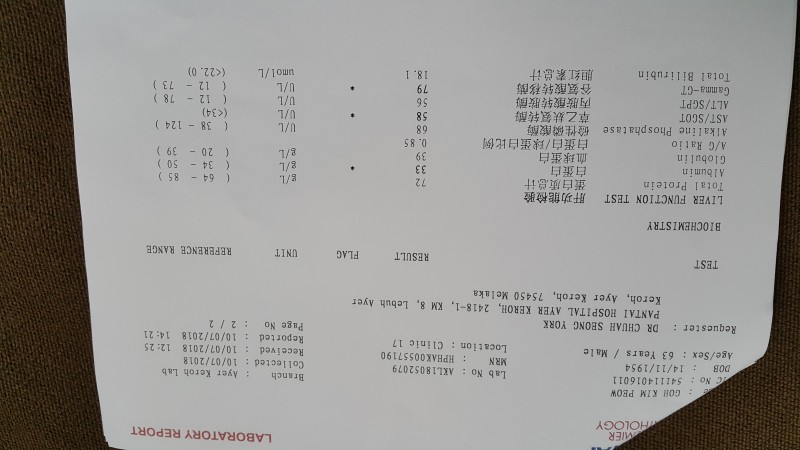
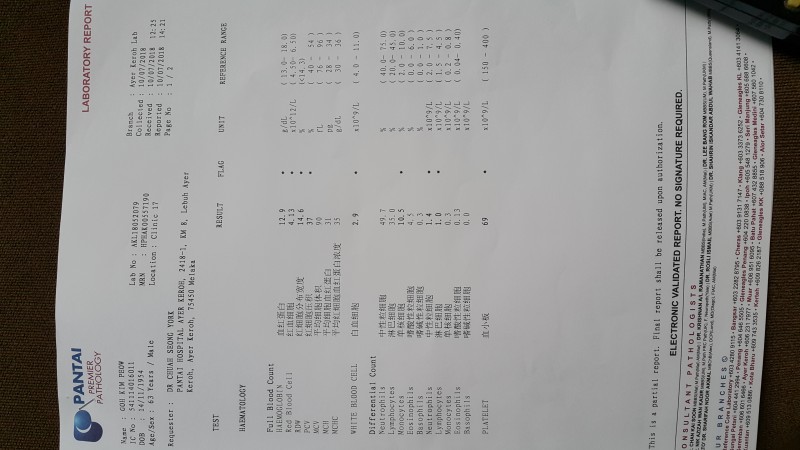
12/6/2018(start treatment) AST 126(<34), ALT149(12~7 , platelet 103
, platelet 103
10/7/2018 (4 weeks after medication) AST58, ALT 58, platelet 69
Do my father stand a good chance of being undetected at 12 weeks ?(although 4weeks VL result is still detected in <12IU/ml) Does my father need to extend treatment for a few more weeks?Attachments:18 July 2018 at 5:02 pm #28352Hello Carolwinnie,
Your father is on a good treatment, however, if it was my father we would be treating for longer than 12 weeks. Most of the extra benefit is adding 4 weeks (maybe 4% extra cure @16 weeks) with another 4 weeks adding 2% extra cure and an extra 4 weeks adding another 1%. The point is that most of the cure is in the first 8-12 weeks, with less and less extra cure the longer we treat.
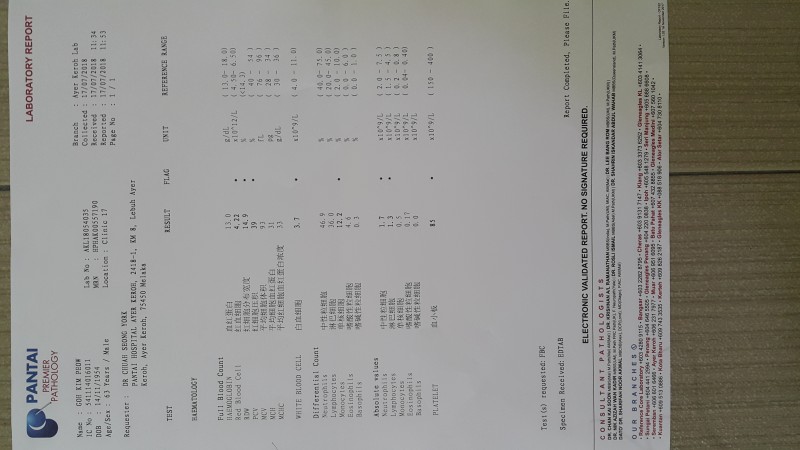
Your father may have to stop the Ribavirin if his platelets continue to fall.
If this happens he should definitely do more than 12 weeks (I would suggest 24 weeks total if we drop back to just using Sof/Vel)
So 12 weeks with Ribavirin is a good treatment for him. He has a good doctor.
Adding extra weeks is good insurance if he is tolerating the drugs well and can be thought of as being like insurance – probably not required, but nice to have if you need it.
YMMV
23 July 2018 at 6:43 am #28362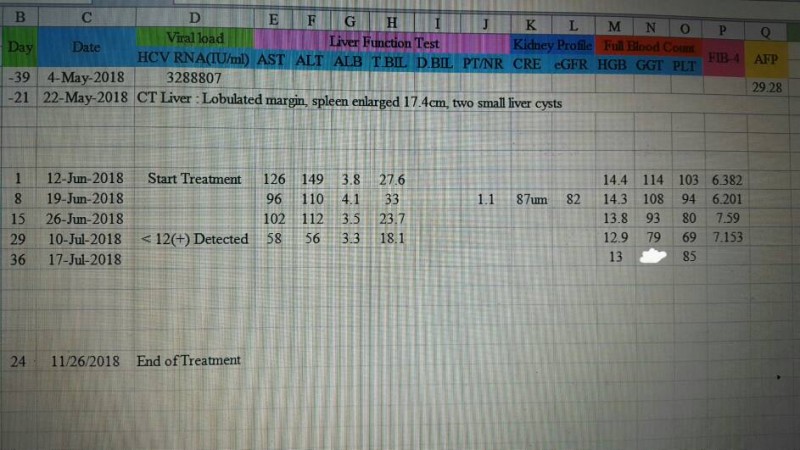
Thanks you very much Dr.James for your suggestions on my father’s medication. Finally, I decide to extend my father’s medication to 24 weeks with what you have suggested.
Here, my other concern is :
My father is decompensated with liver cirrhosis CTP B score 7 . If the next 12 weeks of medication I do not add ribavirin, then approximately at what rate will this outcome be successful?
According to my father’s treatment progress, it is still necessary to add ribavirin?
Thanks you for taking the time to answer me. I am worried about whether my father need to continue ribavirin in the 24weeks treatment.23 July 2018 at 7:59 pm #28364The main benefits of Ribavirin are at the start of treatment so my suggestion would be to use it while side effects can be tolerated (and haemoglobin and platelets remain ok).
If there are problems we can reduce the dose or stop it.
The extra treatment duration is much more valuable to success than ribavirin.
There is not a lot of good data about how successful treatment is in really sick patients (like Child Pugh
https://www.hcvguidelines.org/unique-populations/decompensated-cirrhosis
The main guidance is from ASTRAL-4, where we saw:
https://www.nejm.org/doi/pdf/10.1056/NEJMoa1512614
You will find this table in that paper from NEJM
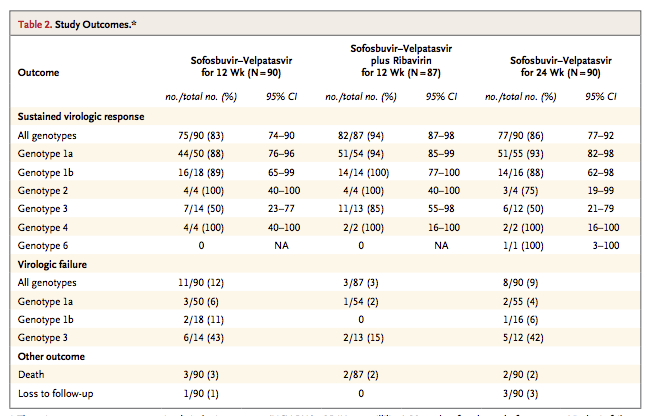
As you can see from the GT3 patients the numbers are small so the confidence interval (margin for error) is quite wide.
For 12 weeks Sof/Vel without ribavirin success was 7/14 patients (50%)
With ribavirin that rose to 11/13 (85%) which is certainly better.
Unfortunately, Gilead did not do 24 weeks either with or without ribavirin but we know from experience what I have already told you – extra treatment duration provides a small, but very real, extra benefit.
I would estimate that with 24 weeks of treatment and at least 12 weeks with Ribavirin we can expect at least a 90% success rate – so 9 chances of success and only 1 chance of failure.
There is nothing better we could be giving. The NS3/4 boosters in Vosevii or Maviret (if combined with Sofosbuvir) or Zepatier (if combined with Sofosbuvir) can not be used in Child Pugh B or C.
You are, in short, doing everything that can possibly be done to maximise the chance of cure.
YMMV
-
AuthorPosts
- You must be logged in to reply to this topic.