
Forum Replies Created
-
AuthorPosts
-
Hello Kaju,
Well the undetected is certainly very good.
Can you share your liver function tests (before starting and now)?
YMMV
3 August 2018 at 5:24 am in reply to: 30 yrs of HepC, 30 day result on Harvoni – Undetectable! #28402Isn’t it amazing how fast the time goes on treatment?
This is a bit different to the post-treatment wait to confirm SVR12 which seems to take forever, but, the odds are solidly on your side at 20:1 in favour.
YMMV
Hello suesp_52,
It’s easier if you post all your results.
Your ALP is fine and slight rises are irrelevant.
Your Urea depends only on how much you drink – more water and it’s lower, less water and it’s higher.
Your CRP is non-specific for anything. CRP goes up with any injury or stress. We should just check it again in a few weeks or if you are unwell we should check you on the merits of that unwellness, not on your CRP value.
YMMV
Wow, how time flies.
It seems like only yesterday we were worrying, and now things are looking great.
It’s important that your boyfriend has regular ultrasounds (every 6 months) of the liver to check for HCC for at least a couple of years, but other than that there is nothing much else that needs to be done.
The new healthy lifestyle sounds good.
YMMV
Great effort Hazel. It’s good to see some non accusatory, why should I bother messaging about why get tested for Hep C.
With the tools shortly to be to hand I can see NZ rapidly catching and overtaking Australia in your elimination efforts.
It is bad enough being beaten in the rugby. With a 2 1/2 year headstart weshould be so much further ahead here.
YMMV
Hi Mark,
Dual genotypes are common and patients are neither sicker nor weller.
Before pan-genotypic treatment like Sofosbuvir+Daclatasvir or Sofosbuvir+Velpatasvir we did see the odd patient treated with Harvoni for GT1 relapse with either GT2 or GT3 (Harvoni does not work for these) so presumably they were dual GT1/2 and GT1/3.
So in short there’s no problem treating and it’s more or less the same as for everyone else with Hep C. You get rid of it and you feel better and your long term health outlook is better.
YMMV
Yes, it makes no difference to cure rates provided the correct drugs are chosen.
Dual genotypes are reported at about a 10% rate in Europe versus 1% in places like the USA. It’s more about the reporting than any real difference.
The actual rate is something like 5-25% so it is common in patients but under reported by pathologists.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4296219/
YMMV
Hello Janet,
Weakness is not something we hear of commonly. Can you explain more about when it started, where, what it is like?
Fatigue is a common and known side effect of the DAA medications.
YMMV
Hi John,
With any luck those things will settle, but there is a difference between association and caused by.
Anyway a blood test will prove the virus is undetectable and liver functions are better so that’s probably not a bad thing to get done to put your mind at rest.
I can’t promise but many things often settle once the Hep C is fixed.
YMMV
Hi John,
When you have Hep C (untreated) it is very difficult to pass it on sexually. Essentially straight sex does not do it. There are stacks of couples where one patient is positive and the other has remained negative for decades while normal sexual activity has gone on.
MSM (Men who have Sex with Men) seem to manage it occasionally, but that almost certainly relates to anal sex.
Once you are on treatment by 4 weeks you are almost invariably (80% chance) undetectable and 99.9% certain to have next to no viral load so the risk of sexual transmission, which was close to zero to start with, is not even closer to zero.
So the basic answer to your questions is no, you are very very unlikely to transmit it.
On the pragmatic front, in new relationships, you are given a “blob” of – largely undeserved – trust. That trust is yours to lose as much as it is yours to prove.
So despite the above you are faced with three practical options
1) Lie and say you are saving yourself until you know her better
2) Lie and pretend the pills are vitamins or hide them…
3) Level up and involve her in the discussion.#1 and #2 are the easy ones and you would probably get away with either
#3 runs the risk of her cutting and running, but, if not, you will have a much deeper relationship and it won’t have started out with a lie you will have to keep to yourself for the rest of your life.
YMMV
The main benefits of Ribavirin are at the start of treatment so my suggestion would be to use it while side effects can be tolerated (and haemoglobin and platelets remain ok).
If there are problems we can reduce the dose or stop it.
The extra treatment duration is much more valuable to success than ribavirin.
There is not a lot of good data about how successful treatment is in really sick patients (like Child Pugh

https://www.hcvguidelines.org/unique-populations/decompensated-cirrhosis
The main guidance is from ASTRAL-4, where we saw:
https://www.nejm.org/doi/pdf/10.1056/NEJMoa1512614
You will find this table in that paper from NEJM
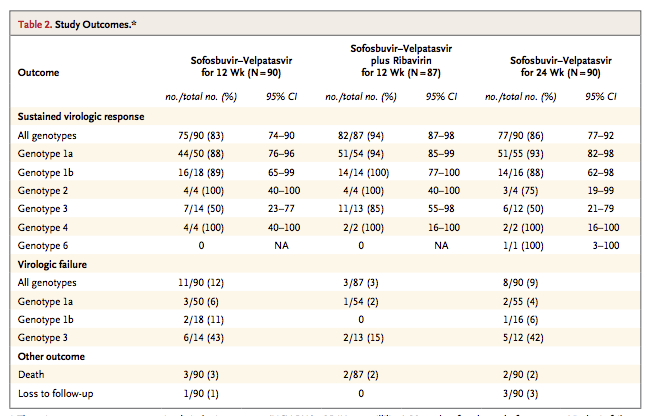
As you can see from the GT3 patients the numbers are small so the confidence interval (margin for error) is quite wide.
For 12 weeks Sof/Vel without ribavirin success was 7/14 patients (50%)
With ribavirin that rose to 11/13 (85%) which is certainly better.
Unfortunately, Gilead did not do 24 weeks either with or without ribavirin but we know from experience what I have already told you – extra treatment duration provides a small, but very real, extra benefit.
I would estimate that with 24 weeks of treatment and at least 12 weeks with Ribavirin we can expect at least a 90% success rate – so 9 chances of success and only 1 chance of failure.
There is nothing better we could be giving. The NS3/4 boosters in Vosevii or Maviret (if combined with Sofosbuvir) or Zepatier (if combined with Sofosbuvir) can not be used in Child Pugh B or C.
You are, in short, doing everything that can possibly be done to maximise the chance of cure.
YMMV
Well how about that! Not bad for something way more heavy going that a funny cat video!
YMMV
Hi Greedfighter,
Article 60 of the World Trade Organisation says members may, rather than must…
Many countries prohibit personal imports.
The FDA rules are here: https://www.fda.gov/forindustry/importprogram/importbasics/ucm432661.htm
And basically say it is illegal except if…
So the reality is that personal inportation is not a right in the USA. It is a discretionary power around the “except if…”
The FDA has been clamping down on it so as you’ve said before – if you are sitting on the fence get yours while the getting is good!
YMMV
Hello Carolwinnie,
Your father is on a good treatment, however, if it was my father we would be treating for longer than 12 weeks. Most of the extra benefit is adding 4 weeks (maybe 4% extra cure @16 weeks) with another 4 weeks adding 2% extra cure and an extra 4 weeks adding another 1%. The point is that most of the cure is in the first 8-12 weeks, with less and less extra cure the longer we treat.
Your father may have to stop the Ribavirin if his platelets continue to fall.
If this happens he should definitely do more than 12 weeks (I would suggest 24 weeks total if we drop back to just using Sof/Vel)
So 12 weeks with Ribavirin is a good treatment for him. He has a good doctor.
Adding extra weeks is good insurance if he is tolerating the drugs well and can be thought of as being like insurance – probably not required, but nice to have if you need it.
YMMV
-
AuthorPosts