
Forum Replies Created
-
AuthorPosts
-
It is lovely to see people who missed out first time round not draw a short straw the second time.
Most people succeed first time.
Sadly a few don’t but as we can see here, and elsewhere, yes it’s a setback, but SVR is still out there and we just have to work a little harder to get there.
Triple drug therapy with an NS3/4A, NS5A and NS5B is the way to go if you can get it.
Adding generic Sofosbuvir to Viekira and Zepatier is the simplest solution where these are available.
Relatively affordable Abbvie Viekira can be sourced out of Egypt if required.
Extended treatment with Sof+Vel+Ribavirin is probably the next best option, but it needs to be done on a case by case basis.
YMMV
Hello Heatherlou30,
The ingredients of oral contraceptives don’t interact.
Here is the interactions report for the standard OCP (ethinyestradiol and norethisterone). Yours has norgestimate (which is not listed in the interactions checker) but is similar to norethisterone.
It will not be a problem, but you can get problems with any medications you take, so do keep us updated if you feel NQR (Not Quite Right).
InteractionsReport2017_05_29_02_32_51.pdf
YMMV
Hello Meri,
There are 5 basic causes of dyspnoea
- Respiratory
- Cardiac
- Blood
- Musculoskelatal
- Neurological
We need to look at all these in turn to find the cause, starting with the most likely.
With the lungs Xray, spirometry (pre and post bronchodilator) and a CT chest would be the starting point.
For the heart and ECG will show rhythm problems and old heart attacks, enzymes are useless in this context as they are only elevated when you have a heart attack for a maximum of 1 week. We do see them elevated with myocarditis (infection/inflammation of the heart) but this is rare. What you need is an echocardiogram (Ultrasound of the heart) to assess valve and muscle function as well as pulmonary pressures.
A full blood count will show anaemia and other blood cell problems. The CMP will look at liver and kidneys.
Musculoskeletal problems are assessed clinically
Neurological things are rare and last on the list.
Here is what the Mayo Clinic has to say about it: http://www.mayoclinic.org/symptoms/shortness-of-breath/basics/definition/sym-20050890
YMMV
Hello J. Eugene,
I know at least one of the generics manufacturers are looking at it. FDA approval has to happen first but it will probably go down as observed before with Bangladesh first and India 6-9 months after FDA approval.
We do have a very good NS3/4A and NS5A combination now – Viekira.
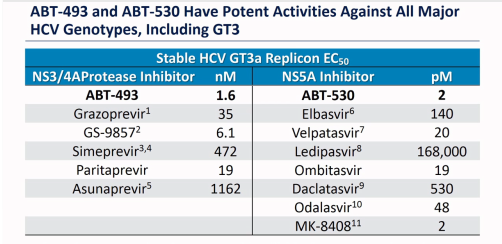
As you can see, in GT3 paritaprevir is almost as good as Vox (GS-9857) and better than the Elbasvir in Zepatier (which is approved for GT3 with Sof). The ombitasvir is just as potent as Velpatasvir and stronger than the Grazoprevir in Zepatier.
On the practical side of things, Abbvie Viekira is marketed in Egypt and can be sourced reasonable affordably, meaning a Sof+Vel+Vox potency combination is available now.
The trials of Sof + Viekira and Sof + Zepatier show it works well:
YMMV
Hi RSF,
Hopefully it’s not, but if it is we will just have to fix it won’t we?
YMMV
While this site from Gilead suggests limiting caffeine: http://www.harvoni.com/discover-harvoni/common-side-effects
The official product literature: https://www.gilead.com/~/media/Files/pdfs/medicines/liver-disease/harvoni/harvoni_pi.pdf
Does not mention it.
Caffeine has been shown to delay development of fibrosis and life without coffee would render me dysfunctional and sad so I can find plenty of reasons to go with literature #2 rather than #1
YMMV
25 May 2017 at 8:50 am in reply to: Can Pharma companies produce enough DAAs to erradicate HCV? #26166Another way of looking at it is like this.
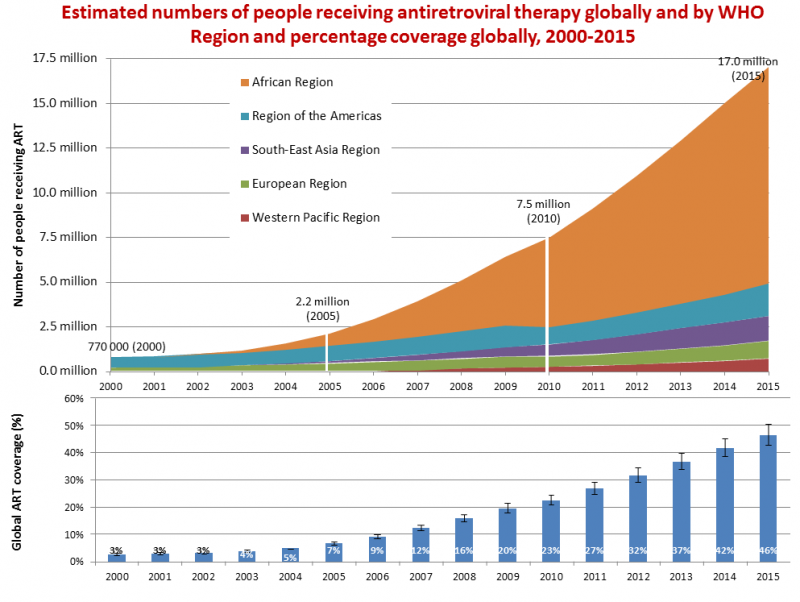
The WHO estimate has dropped to 70 million with HCV.
Currently, we treat 17 million patients with HIV with 52 weeks of double, triple or quadruple antivirals.
These antivirals are similar to HCV antivirals.
So 17 million full year treatments are the same as 17*52/12 = 73.6 million 12 week treatments.
In short we have proven capacity to make enough antiviral medicine for every patient in the world with HCV in a single year. We already produce more than this quantity for HIV.
It took us 10 years to get to that scale, but still, it is quite clearly doable without raising much of an industrial sweat.
YMMV
The episodes are here on ABC iView for about another 2-3 weeks (they are available for 28 days after broadcast)
Promos:
Part1 http://www.abc.net.au/austory/content/2016/s4665628.htm
Part2 http://www.abc.net.au/austory/content/2016/s4670742.htmFull:
Part1 http://iview.abc.net.au/programs/australian-story/NC1701Q014S00
Part2 http://iview.abc.net.au/programs/australian-story/NC1701Q015S00
YMMV
That’s fabulous news Coral


YMMV
Take 12 weeks!
mWhat he said!
YMMV
Hello 2b,
While there is no good guidance on this, in mg/kg terms you are getting the same dose as somebody of about 70kg. We don’t consider dose increases for 80, 90, 100, 100 kg patients so if things seem better on this slightly reduced dose I think it should not impact treatment success.
As an experiment, if you take the full tablet for a day or two and the problems recur that would be compelling evidence we are giving you just a little too much.
YMMV
Hello 2b,
Any update?
YMMV
.
HCV RNA consists of 9600 bases. Each weighs about 650 Daltons and 1 Dalton is 1.67 x 10-24grams so you could multiply all those together and get a really small number – about 10-17 grams.That’s really really really really really really really really really really really really really really really really really small.
0.00000000000000001 g
We use the process PCR – which is Polymerase Chain Reaction like this. We add some blood that may have RNA in it to a chemical soup of RNA duplicators. We incubate it to make lots of RNA, and only now do we have enough to count.
So that is problem 1.
Problem 2 is that it only takes about 10 Hep C virions (viuses) to cause infection.
If these were all in your blood, and there were only 10, and you have 5 litres of blood (you do) then we would need to draw off 500 ml to have a chance of getting 1 virus. We only take 5 ml.
And of course most of the HCV is NOT in your blood – it is in liver and other cells.
So while it would be great to measure down to zero it is fundamentally impossible to do so because:
- We can’t measure small enough
- We can’t take enough blood, you would die
- And there is more virus not in the blood that we simply can’t get at – we would have to homogenise at least 10% of you in a blender per test
YMMV
We try to keep things off politics here, but there are a few historical lessons relevant to us all.
The problems we are seeing today trace back to Raeganomics which was essentially de-regulate and drop taxes.
https://mises.org/library/sad-legacy-ronald-reagan-0
The problem with de-regulation, particularly in banking was that those regulations were put in place in the aftermath of the great depression. Sadly the lessons learned back then had been lost in the sands of time and the repeal of various regulations allowed the housing crash in the USA to happen.
Many of the leaders who have followed Raegan have done similarly. This article is titled “Trump’s proposing big tax cuts. Here’s what history says happens next”
https://www.linkedin.com/pulse/trumps-tax-cuts-may-more-damaging-than-reagans-steven-rattner
You have to go, hey, it’s never worked before, so why do you think it will work now?
In 1950 Frank W. Abrams, chairman of Standard Oil of New Jersey, voiced the corporate mantra of “stakeholder capitalism”: the need to balance the interests of all the stakeholders in the corporate family. “The job of management,” he wrote, “is to maintain an equitable and working balance among the claims of the various directly affected interest groups,” which he defined as “stockholders, employees, customers and the public at large.”
We don’t hear that sort of sentiment anymore. It is all about maximising profits for shareholders (and CEOs) and Gilead is simply a symptom of that, not the root cause.
http://www.nytimes.com/2012/09/03/opinion/henry-ford-when-capitalists-cared.html
YMMV
Hello Gert,
Yes, there are studies. You want page 18 of the EASL Guidelines (see PDF) that reports the major studies used for the guidelines and provides references for them you can then look up.
SOF+VEL: ASTRAL-3
Short version: http://slides.hcvonline.org/uploads/194/astral3.pdf
Long version: http://www.nejm.org/doi/full/10.1056/NEJMoa1512612#t=articleSOF+DCV: ALLY-3 and ALLY-3+
Short version: http://slides.hcvonline.org/uploads/164/ally3.pdf
Long vesion: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4409820/ALLY-3+ https://www.ncbi.nlm.nih.gov/pubmed/26822022
There is another bigger SOF+DCV trial here: http://fixhepc.com/forum/gt3/369-gt3-high-svr-rates-with-daclatasvir.html which includes a PDF of the results. It does not have a funky name AFIK.

You may notice that the results for SOF+DCV vary a bit and include similar optimistic numbers to SOF+VEL
Now this table is interesting (and you won’t easily find it). It comes from Abbvie who were talking about how good G/P is (previously called ABT-493/ABT-530). GS-9857 is Voxilaprevir in case you’re wondering.
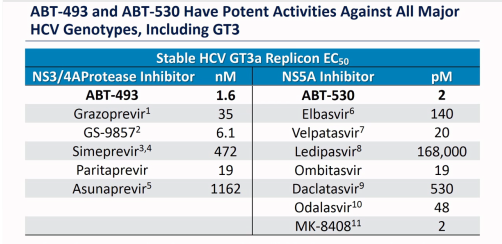
In theory Velpatasvir should be better – It has an EC50 of 20 vs 530 for daclatasvir, but only about 25% gets absorbed so that robs it of part of the 26.5x theoretical edge, dropping it to say 7x, but then the dose is 100 mg vs 60 mg so that pushes it up to about 10x.
Now resistance comes in 10x, 100x and 1000x strengths so 10x is just enough to probably make a real difference for a few patients.
I have no doubt that 16 weeks SOF+DCV works better in GT3 patients than 12 weeks, so that is a factor.
Attachments:
YMMV
-
AuthorPosts