
Forum Replies Created
-
AuthorPosts
-
30 March 2016 at 4:47 pm in reply to: relapse cases : is it due to advanced fibrosis or cirrohsis? #14641
Hi Tweak,
In the real world getting 100% is really hard. The contraceptive pill is very effective but results are 97%. There are many issues.
Genotype
GT2 is probably the easiest to clear – 97% with Sof+Riba beat all the other genotypes. GT1b is easier than GT1a. GT3 is much harder than GT1.
Compliance
I have a GT2 patient who is a SVR4 but he took 4 weeks Sof+Dac, had 2 weeks off, took another 4 weeks then stopped and still has the last 4 weeks. He was just lucky.
I have another patient who went on holiday, forgot his tablets, did not take for 2 weeks in the middle but completed 12 weeks over 14 weeks. He has relapsed, and probably did himself no favours. I have another with the same profile and pending results.
When I ask patients about this I don’t say “did you take all the pills” I ask “how many pills did you miss” because most people do miss a few.
Absorption and Dosing
Some patients taking a small dose of drug have high blood levels – take warfarin as an example – for some patients 1-2 mg a day is enough for others 10 mg is required. We use fixed doses, with no weight adjustment – big people get less mg/kg of drug than small people. At least one relapse I know if was well over 100 kg and perhaps under dosed.
With daclatasvir we seem to have identified Taurine in Red Bull and other energy drinks as a problem by inducing CYP3A4 and lowering the daclatasvir levels. Some supplements people take may not be helping.
Coinfection
Although it is not talked about in the english literature a lot coinfection exists. It makes sense that someone exposed once may have been exposed twice, and while one genotype may dominate you could still have low levels of another. Say you have GT1 as the main type and GT3 at low level and take Harvoni – this is not so good for GT3 and there are reported cases of GT1 relapsing as GT3 – one explanation is re-infection – another is coinfection inadequately treated
Response and Resistance
We have seen on treatment virological breakthrough in 2 patients and both behaved like patients on NS5A monotherapy with a slow viral load decline then relapse. It was like the sofosbuvir was not working. This is entirely possible and could be due to NS5B resistance, but my theory is that the sofosbuvir pro drug (which requires 2 phosphorylation steps to become active) was not phosphorylated by CatA and/or CES1 enzymes – deficiencies of both these enzymes are reported.
NS5A RAVs also exist at baseline and are more common in patients that relapse.
Fibrosis
For GT1 fibrosis does not seem to make a huge difference but for GT3 it definitely does. Some people’s fibroscans are out of date and they may have not been given sufficient duration.
Past Failure
With GT1 past failure reduces the 97% SVR to 94% with 12 weeks treatment. This increases to 96% with ribavirin or 99% with 24 weeks treatment.
Notice that the extension by 12 weeks only gets an extra 5% in this case.
Viral Load and Innate Immunity
With GT1 we know that with low fibrosis and treatment naive the SVR rate is excellent with 8 weeks treatment (98%) if the viral load is < 6 million, but over 6 million and 8 week SVR rate is 90%. More virus probably means more mutations to deal or more to kill or that the patient needs more help (as their immune system is basically ignoring the infection). Whatever the reason we need longer, at least for GT1, with a high viral load. Genetics
As well as the possibility of CatA and CES1 defficiency there are probably many other factors.
IL28 is not commonly considered but may have a mild impact with CC people more sensitive to the body’s natural interferon than CT or TT people.
What is required
If a researcher inject 10 virus particles into a monkey they might get an infection. If it is 100 virus particles they WILL get an infection so we really need to kill just about every last virus on treatment.
So there are many possible reasons for relapse.
Longer, stronger and different drugs are the suggested approach to retreatment.
YMMV
Fibroscan is better.
APRI score seems pretty good with predicting people who are close to or at cirrhosis and should run longer.
YMMV
Your platelets and APRI score suggests you may be more than F1. If you can afford it an extra 4-6 weeks is not a bad idea.
YMMV
What were your platelets, AST and ALT before treatment?
YMMV
Hi A
I have completed my treatment and am just waiting on my SVR12 blood test to be done in four weeks. Undetected so far!!
I also had insomnia most of the way through treatment but my general energy levels were so much better. I did get used to the insomnia and it didn’t trouble me too much at all.
You are in very good hands. All the best for your treatment.
Cheers
Lynne

YMMV
Do 24 weeks Sof + Dac, no Riba.
Riba will take 94% SVR for a prior treatment failure GT1 patient to 96% SVR on a 12 week treatment but given you can have 99% SVR with 24 weeks without Riba unless you (personally) need to save the money you as an individual patient are far better off running with 24 weeks.
We will publish the SVR data for generics on 16th April at EASL, but if you want to get started use the treatment advice above.
Glad you like the tool!
YMMV
Hi Serg,
24 weeks Sof/Led or Sof/Dac alone should give you a 99% SVR probability.
- F4 is a weak negative predictor.
- High viral load (assuming you are > 6 million) says definitely do 12 not 8
- Past failure is your major issue as it drops the 97% SVR to 94% @12 weeks but this pulls up to 99% @ 24 weeks.
As you note there is a slightly different resistance profile for Led and Dac. You already have all your RAVs even if we can’t measure them. These drugs are not mutagenic, they simple expose RAVs by selection.
Please note that the following advice has relatively little proven scientific basis (in trials data) but if you’re going to do 24 weeks – and that is the right choice – then 12 weeks Sof+Dac and 12 weeks Sof+Led gives you 24 weeks Sof + exposure to 2 different NS5As, so if you have a few mutants left at the end of the first 12 weeks, the second 12 weeks should do the job on these stragglers.
1b is the easiest to clear, so you are looking at great odds without Asunaprevir.
Asunaprevir, like all NS3/4 agents, is a bit toxic. I would suggest keeping it up your sleeve as the Plan B if the 99% odds of 24 weeks of 2 DAAs don’t work for you.
I would not bother with the Ribavirin. It will add little or nothing to your SVR probability on a 24 week treatment course, but it will make you suffer during treatment.
If you go here: http://fixhepc.com/hcv you will find a tool that contains the EASL and AASLD guidelines, but more importantly if you put in your numbers and then use the “Show Trials” button at the end of the results it will show you pretty much everything that is known in terms of hard data.
YMMV
For Sof + Led late in the evening probably gives best absorption. For Sof + Dac it probably does not matter. It seems to work regardless.
YMMV
Ledipasvir absorbs better in acid conditions. PPIs and H2 antagonists have the same impact.
The original research data showing the absorption issue was in dogs primed with famotidine – another H2 antagonist.
It is best to use Sof+Dac if you need to use any antacid medications.
You are taking Sof+Dac so can take as much or as little Ranitidine as you require when you require it.
YMMV
27 March 2016 at 3:56 am in reply to: Has Buyers Club been closed by the Australian government? #14518On the 19th of December 2015 the Australian Government blocked air cargo into Australia from a number of countries, including Bangladesh
https://infrastructure.gov.au/security/air-cargo/prohibition-intl.aspx
Coincidentally this happened at the same time that the Australian Government announced these medications would be put on the PBS making the need for something that worked in Australia only more or less non existent.
REDEMPTION has the capacity to scale and is reliably delivering Indian generics around the world.
The clinical results of generics – Chinese, Bangladesh and Indian, are under embargo until EASL but it would be reasonable to assume that the right medication given to the right patient for the right duration should deliver predictable results.
YMMV
- You are taking too much Ribavirin. The correct dose for your weight is either 800 mg or 1000 mg total each day in 2 divided doses (this assumes you have normal renal function. I suggest reducing the dose immediately.
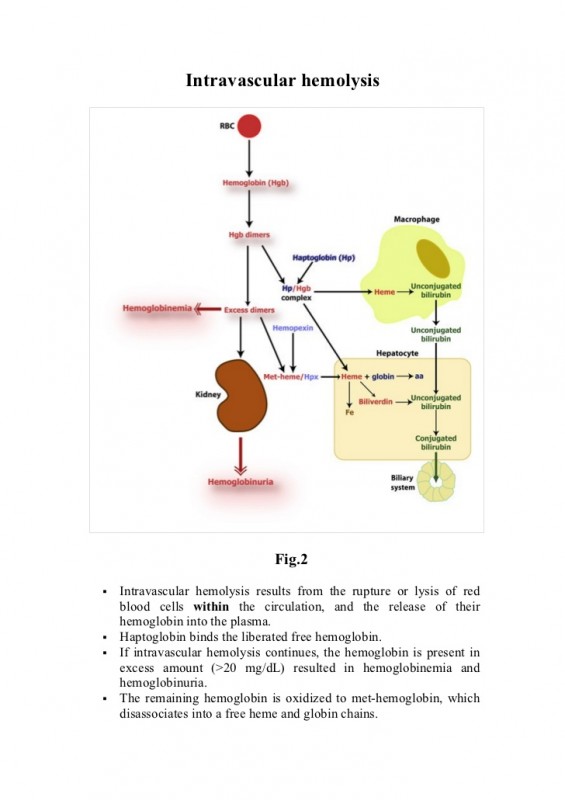
- Ribavirin can cause a haemolytic anaemia – haemolytic means that red cells “explode”
- When red cells break down they release stuff that becomes bilirubin
YMMV
My GP informed me a couple of weeks ago that he will be on board with prescribing the meds but he will be doing a couple of “courses” first to learn more about them and what he needs to know to prescribe them. He has been awesome all the way through with me and has been a great support albeit not knowing all that much about the generics at the time. He has faxed all my results to James (as he requested) and has been more than helpful if I have any questions. I have a smidge over four weeks to go before I get my blood test for SVR12. Fingers crossed
YMMV
Sorry to hear Paul..I’m sure your next lot of treatment will see the end of this rotten virus….good luck.
YMMV
-
AuthorPosts


