Hi Sven,
While laboratories tend to report a single genotype, about 10% of people are probably infected with 2 genotypes:
www.ncbi.nlm.nih.gov/pmc/articles/PMC4296219/
www.ncbi.nlm.nih.gov/pmc/articles/PMC3205070/
We have seen people treated for GT1a with Harvoni relapse with GT3 despite a negligible reinfection risk so presumably, they had both GT1a and GT3, and the Harvoni only cured the GT1a leaving the GT3 to flourish.
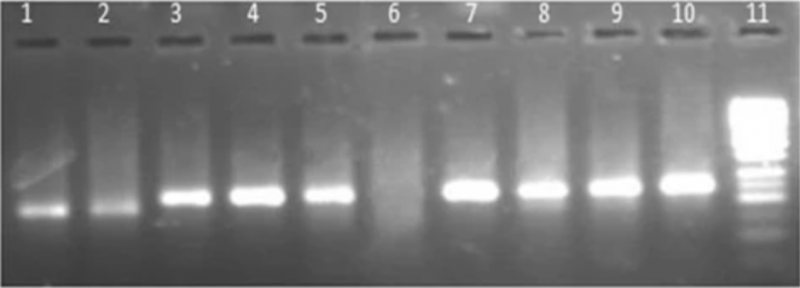
Here is an image of some actual genotype testing:
Lanes 1 and 2 are GT1. Lanes 3-5 and 7-10 are GT3. Lane 6 is negative. Lane 11 is the control.
Look carefully at lane 8 and notice that while GT3 is dominant there is a clear GT1 line below it. Some of the other GT3 lanes also suggest GT1 but lane 8 seems pretty clear. That result would be reported as GT3 but is really GT3/GT1
So, it is possible that somebody infected with 2 genotypes can pass on both, and that in the other person a different genotype is the dominant one.
Ledipasvir is not effective against GT2 or GT3 so, for a patient coinfected with GT1/GT2 or GT1/GT3 the Harvoni should cure the GT1 but there is only a 70% chance of curing the GT2 or GT3 (because Sofosbuvir alone has about a 70% cure rate for these).


{kind=link}