My personal view is that the thinking on resistance is wooly.
HCV is a quasi-species meaning that it mutates pretty rapidly. Each replication cycle brings the a possibility of roughly 1:10,000 of creating a mutant. Once this is created it exists. If it can't reproduce it dies. If it can, and it is resistant then it will take it's place in the population according to its fitness. If it is very fit we may be able to see and measure it (fit means makes lots of kids fast), but if it is less fit we won't be able to see and measure it.
THE FACT THAT WE CAN'T SEE ENOUGH TO MEASURE DOES NOT MEAN ITS NOT THERE!
The key point is the the CREATION of resistance requires replication, so it happens BEFORE treatment starts unless we don't get good viral suppression and replication continues.
When we treat we kill of the easy to kill virus and suppress almost all replication. With no replication there is no opportunity for a mutation to form.
Virus that already existed, that is resistant will not be killed efficiently, although it's growth will not be helped by the drugs. Nevertheless it will survive and when we remove the drugs it grows back. Now we can see it and measure it, but it was not created by treatment. It existed before we started.
In HIV we know that resistance occurs in the context of ongoing replication.
www.ncbi.nlm.nih.gov/pubmed/19048205
HIV is an unstable RNA virus like HCV so the lessons there apply here. And the lesson for retreatment should be hit the virus as hard as possible to suppress replication (ie add Riba and or a 3rd DAA) so that an already partly resistant virus can not add more resistance mutations to the same strand of RNA.
Anyway those are my thoughts. I expect conventional wisdom to catch up in due course. As you can see from the abstract above this idea is known, it just does not seem to get talked about much in HCV circles.
The reason for waiting to retreat is, to me, not to wait for RAVs to fall to levels we can't measure. They will still be there, probably forever. It is to wait for access to more powerful drugs, or preferably extra agents
The advantage of a 3rd agent
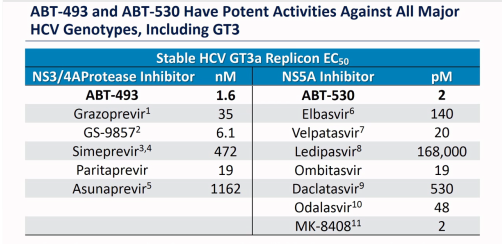
RAVs deliver a 10x 100x or even 1000x resistance to drugs. What this means is that the EC50 (Effective Concentration to kill 50%) of a better drug needs to be 10x + to make a real difference. Let's look at GT3 EC50:
We can see for example that Velpatasvir needs 20 pM to get to EC50 and Daclatasvir needs 530 pM so VEL is 26.5x more potent than Dac. However this is in a test tube. 75% of VEL is excreted unchanged in faeces so it is possible it's not absorbed (the literature speculates on this). That might well reduce the 26.5x to more like 7x. Anyway if you look at the potencies you can see that even for the best in class ABT-530 (that you can't get) it is at best 250x better than DCV. This is good, but still leaves the 1000x resistance variants as problem children.
Ok, now consider a 3rd good drug.
If the probability of creating 1 resistant variant is 1:1000 (it's lower than this but let's use this) the probability of getting 2 resistance variants in the same bit of RNA is 1:1000 x 1:1000 which is 1:1,000,000. Now if we add a 3rd agent the virus now needs to have 3 resistance sites in the same strand of RNA and the chances of getting that are 1:1000 x 1:1000 x 1:1000 or 1 in a billion. Notice that the extra drug adds what you might call 1000 units of power, whereas even the best most potent new drug add 250x
Conclusion: 3 drugs beats 2 drugs.
Validation: In HIV we start with 1 drug: AZT and it works but resistance is rapid. Then we get ddI and ddC
www.ncbi.nlm.nih.gov/pubmed/19048205
And we find that 2 drugs beats 1 drug. And nowadays with lots of agents HAART (Highly Active Antiretroviral Therapy) with 3 or even 4 agents is the standard of care.
HCV is an RNA based virus like HIV. Yes it does not have a reverse transcriptase but the core genome is RNA so lessons from HIV are broadly applicable.
Validation2: Viekira-pak is a very effective existing poly target treatment, and as the QUARTZ-1 trial shows adding Sofosbuvir to it makes it outstanding. C-SWIFT is adding SOF to Zepatier's NS3/4A + NS5A combination.
www.aidsmap.com/Treatment-intensificatio...atment/page/3014995/ 

") , no ofense dr. F)
, no ofense dr. F) ( Meds stopped after 4 or 5 months.
( Meds stopped after 4 or 5 months. .
.



{kind=link}