
Home › Forums › Main Forum › Media & News › Research and Trials › Abbvie ABT-493/ABT-530 gets FDA breakthrough therapy designation
- This topic has 7 replies, 4 voices, and was last updated 9 years, 3 months ago by
 Dr James.
Dr James.
-
AuthorPosts
-
20 October 2016 at 12:14 pm #23963
Abbvie’s new pangenotypic Glecaprevir/Pibrentasvir NS3/4a + NS5a combination has been awarded breakthrough designation based on results of phase 2 trials with GT1 patients who had previously failed DAA treatment. They will apparently also be presenting pangenotype phase 3 trial results at AASLD in Nov.
Probably still a way off but so far looks promising for relapsers in the future.
G3a since ’78 – Dx ’12 – F4 (2xHCC)
24wk Tx – PEG/Riba/Dac 2013 relapsed
24wk Tx – Generic Sof/Dac/Riba 2015/16 relapsed
16wk Tx – 12/01/17 -> 03/05/17 NS3/NS5a + Generic Sof
SVR7 – 22/06/17 UND
SRV12 – 27/07/17 UND
SVR24 – 26/10/17 UND
 21 December 2016 at 12:13 pm #24780
21 December 2016 at 12:13 pm #24780Glecaprevir pibrentasvir will probably get FDA approval soon. https://news.abbvie.com/news/abbvie-submits-new-drug-application-to-us-fda-for-its-investigational-regimen-glecaprevirpibrentasvir-gp-for-treatment-all-major-genotypes-chronic-hepatitis-c.htm
Abbvie filed for FDA approval, days after Gilead. The timeframe is about 8 months.
This combination is even more potent than sof/vel/vox for retreatment, has a different resistance profile.
That said, sof/vel/vox does have 97% SVR for retreating many cases.
The more different drugs for retreatment – the better. Some failed combinations require retreatment with drugs having a different mechanism of action and resistance profile. And if one doesn’t work, it may be good to try chances with another one (although, there’s debate if one should wait for a year before retreatment, especially when one has a s282t rav).I wonder who will be the first one to copycat it. The retreatment market is about 18 million people – and there are no good options on the market currently.
Gen 1b
VL pre treatment 29000 ME/ml
AST 32 ALT 94, F0
Started treatment 13 January 2017
Generic sofosbuvir/velpatasvir (Incepta)
VL 9 days into treatment <300 (undetected)
AST 13.8 ALT 22
Side effects: mild dehydration, not a problem at all if I drink water at night, nothing to worry about
Diet and gastric ph are very important with velpatasvir. One must think what and when to eat to keep gastric pH low. Side effects disappeared 2 weeks after, unless I ate anything < 4hrs before the pill. SVR60.21 December 2016 at 4:37 pm #24781Hi Vitrus,
Thanks for posting. It’s reassuring to see that they have submitted the application for approval. When it is approved it will no doubt provide another option for retreatment that will be particularly useful for ‘difficult to treat’ patients. Ideally this and other new and more effective meds will also be available for treatment naive patients too, which will reduce the numbers who need retreatment. And that will be a great news!

However, while retreatment can be problematic for some of us currently I would also suggest that there are some good options already available in the currently approved/available medications depending on the patients genotype and/or other issues such as cirrhosis, etc.
G3a since ’78 – Dx ’12 – F4 (2xHCC)
24wk Tx – PEG/Riba/Dac 2013 relapsed
24wk Tx – Generic Sof/Dac/Riba 2015/16 relapsed
16wk Tx – 12/01/17 -> 03/05/17 NS3/NS5a + Generic Sof
SVR7 – 22/06/17 UND
SRV12 – 27/07/17 UND
SVR24 – 26/10/17 UND
25 January 2017 at 1:46 am #2512899% SVR in Japanese CERTAIN-1 trial (January 2017) of glecaprevir/pibrentasvir.
(Gen 1 only, 8 weeks, 106 people).
The 1 remaining percent is one patient lost to follow-up.
http://www.businesswire.com/news/home/20170109005300/en/Enanta-Announces-High-SVR12-Rates-Achieved-GenotypeIn previous November trials, SVR12 in 97.5% people across all genotypes.
https://news.abbvie.com/news/eight-weeks-treatment-with-abbvies-investigational-pan-genotypic-regimen-glecaprevirpibrentasvir-gp-achieved-high-svr-rates-across-all-major-genotypes-chronic-hepatitis-c.htm
Gen 1b
VL pre treatment 29000 ME/ml
AST 32 ALT 94, F0
Started treatment 13 January 2017
Generic sofosbuvir/velpatasvir (Incepta)
VL 9 days into treatment <300 (undetected)
AST 13.8 ALT 22
Side effects: mild dehydration, not a problem at all if I drink water at night, nothing to worry about
Diet and gastric ph are very important with velpatasvir. One must think what and when to eat to keep gastric pH low. Side effects disappeared 2 weeks after, unless I ate anything < 4hrs before the pill. SVR60.25 January 2017 at 2:53 am #25132While these results are encouraging it’s worth noting that most Japanese are GT 1b which, along with GT 2, is the easiest GT to clear.
Gilead’s 97% SVR for GT1 with Harvoni in 300 or so treatment naive low fibrosis patients in ION was shown to be 91.3-92% in a VA study of 4200+ real world veterans. The slightly higher result being in the with Ribavirin group.
What’s good about these new drugs is that they are the most potent NS3/4 and NS5A inhibitors to date. Looking at GT3 we see this:
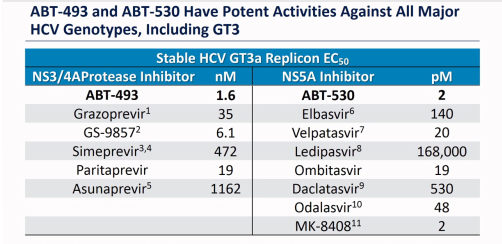
So ABT-530 needs 2 pM for EC50 whereas Daclatasvir needs 530 pM. That 265 x increase in potency is enough to deal with RAVs that confer 10x and 100x resistance (but not 1000x resistance). Similarly ABT-493 is 4x more potent than GS-9857 (Voxilaprevir).
To me the most exciting thing is that ABT-493 + ABT-530 + Sofosbuvir looks an awful lot like the mythical Perfectovir. Best in class inhibition at 3 different target sites.
One of the depressing things about ~90% cure is the sure knowledge that 10% will fail. Retreat and get 90% cure and overall we are at 99% but that missing 1% is still 1 real persons hopes and dreams per 100. These new agents offer real hope for cure for almost everyone.
YMMV
15 February 2017 at 10:26 pm #25318FDA grants priority review designation to glecaprver/pibrentasvir.
It means it may get registered in the US late June.
Canada and the EU also recently granted it expedited review for approval.
Gen 1b
VL pre treatment 29000 ME/ml
AST 32 ALT 94, F0
Started treatment 13 January 2017
Generic sofosbuvir/velpatasvir (Incepta)
VL 9 days into treatment <300 (undetected)
AST 13.8 ALT 22
Side effects: mild dehydration, not a problem at all if I drink water at night, nothing to worry about
Diet and gastric ph are very important with velpatasvir. One must think what and when to eat to keep gastric pH low. Side effects disappeared 2 weeks after, unless I ate anything < 4hrs before the pill. SVR60.17 February 2017 at 4:17 pm #25335Are these two drugs going to be produced in Bangladesh?
GT 3a
Contracted: October 2008
Diagnosed: March 2009
First treatement:
VL 250.000 IU/ml
Fibrosis F0
Start: November 2010
Copegus+Pegasys (24 weeks)
EOT: VL UND
SVR24: VL DETECTED
June 2016
Fibrosis F2 (9.1 kPa)
VL 1.230.000 IU/ml
Second treatement:
SoviHep+DaciHep (24 weeks)
Start: 13.08.2016
VL UND: 30.08.2016
VL UND: 27.01.2017 (EOT)
EOT+4 weeks: AlAT 9.8 SVR4
EOT+8 weeks: AlAT 9.7
EOT+12 weeks: AlAT 7.0
EOT+28 weeks: AlAT 7.6 SVR2818 February 2017 at 7:07 am #25340 -
AuthorPosts
- You must be logged in to reply to this topic.