Forum Replies Created
-
AuthorPosts
-
This is what you see when
1) You have been exposed to Hep B
2) You have created your own immunity (Hep B surface antigen) and cleared the infectionSo you don’t have chronic Hep B and should be at minimal (?no) risk of reactivation.
YMMV
It sounds like you are contemplating getting API direct from somewhere.
Please be aware there is a lot to know that you probably don’t, but to answer the question directly you are looking for:
Sofosbuvir CAS 1190307-88-0
Daclatasvir 2HCl CAS 1009119-65-6
Ledipasvir Acetone CAS 1441674-54-9Please note that Sofosbuvir is free base so dose is 400 mg and 34g of API is required for 12 weeks
Daclatasvir is the 2 HCl (2 hydrochrloride) salt and requires 66 mg of API to deliver 60 mg of Daclatasvir and 5.6g of API is required for 12 weeks.
Ledipasvir acetone requires 96 mg of the API to deliver 90 mg of Ledipasvir and 8.1g of API is required for 12 weeks.
Special measures need to be taken to increase the solubility of Ledipasvir. Unless you understand this you would be best off to use Sofosbuvir and Daclatasvir – it’s cheaper and in our testing equally effective in GT1 as well as being pan-genotypic.
YMMV
Please have a look over here:
If you have seroconverted and generated Hep B Surface ANTIBODY you should be fine.
I’ve moved this over to Q&A
YMMV
You are welcome. At F4 waiting is not a great plan – we are running out of wiggle room.
YMMV
They are not ILLEGAL, they are merely unapproved – 1:14
As true as it was then as it is now.
[video]https://www.youtube.com/watch?v=fvMPU0WaPcc[/video]
YMMV
I am a 50yr old male, live in NZ and have HCV Genotype 1A.
I’m classed as a responder / relapser from a past 48week treatment of Pegulated Interferon & Riavirin.
December 2013 Fibroscan has shown fibrosis at F4.
I now have cirrhosis.12 weeks Harvoni gives you a 94% SVR (the past failure has more impact than the cirrhosis). If your platelets are > 100 and you’re up for it 12 weeks with Riba moves that up to 96% but you will need monitoring every 2 weeks for the expected anaemia, etc. 24 weeks without Riba should deliver 99% odds.
If money was no object doing a full 24 weeks without Riba would be the gold class option, but 94-96% odds are still pretty good.
Sofosbuvir Ledipasvir
NAIVE
default: svr: 97%, trials: ION-1 98% (142/145) ION-3 96% 96% (165/172) Aggregate 96.8% (307/317)
gt1a: default: svr: 97%, trials: ION-1 98% (142/145) ION-3 96% 96% (165/172) Aggregate 96.8% (307/317)
gt1b: default: svr: 99%, trials: ION-1 100% (67/67) ION-3 98% (43/44) Aggregate 99.1% (110/111)
F4
default: svr: 97%, trials: ION-1 97% (32/33)
w12: svr: 97%, trials: ION-1 97% (32/33)
w12riba: svr: 100%, trials: ION-1 100% (33/33)
w24: svr: 97%, trials: ION-1 97% (31/32)
w24riba: svr: 100%, trials: ION-1 100% (36/36)
FAIL
default: svr: 94%, trials: ION-3 94% (102/109)
w12: svr: 94%, trials: ION-3 94% (102/109)
w12riba: svr: 96%, trials: ION-3 96% (107/111)
w24: svr: 99%, trials: ION-3 99% (108/109)
w24riba: svr: 99%, trials: ION-3 99% (110/111)
YMMV
There is another thing happening in NZ. Tina mentioned that…..
In NZ we have a popular soap (much like Neighbours – Home and Away) called Shortland Street. 2 days ago they have introduced a Hep C story line where one of the core characters ( a surgeon) gets a needlestick injury from transferring blood into vacutainers. From the looks of things it’s going to be a big story line and Shortland Street does a good job of educating about medical conditions.
YMMV
Hello PKQ,
How about you see me online, we make the right prescription and you can revisit him cured by June?
YMMV
Ok, once you have the positive antibody you are cured and can do DAA without any fears of any reactivation?
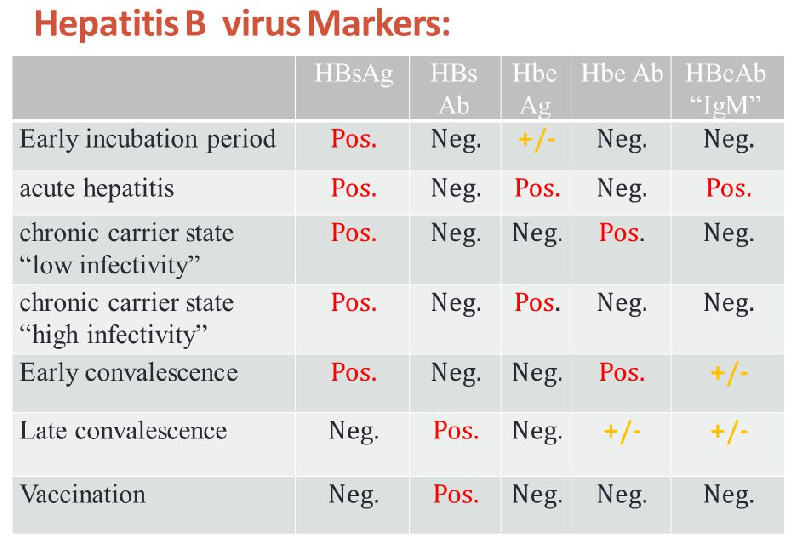
There are antibodies to surface, core and e.
The protection to infection comes from surface antibody so that’s the one you want and you can get it from either vaccination OR infection with natural immune clearance. Chronic Hep B is characterised by failure to develop effective levels of surface antibody.
The correct screening is to do all 3 of:
- Surface Antigen
- Surface Antibody
- Core Antibody
From which you can work out a person’s status, however if you just want to know immune/non-immune status and don’t care if it is vaccination or past infection that triggered it then surface antibody will do.
YMMV
In small quantities and on a not-every-day basis you can eat just about anything.
The only patients I’m aware of who have got into a bit of trouble have been creatures of daily habit – paw-paw every day, grapes every day…..
All that happens with CYP3A4 inhibitors is that you end up with higher blood levels of daclatasvir. This would be expected to be slightly more effective BUT at the expense of more side effects. The dose of 60 mg chosen is because it’s about the strongest the average person can take and good enough to do the job.
YMMV
You want a positive Hep B surface Antibody. You get this from immunisation or infection with natural clearance.
YMMV
20 March 2016 at 5:00 am in reply to: where is the drug interaction site for easy access – please post #14246The GP cheat sheet contains links to pretty much everything needed including the interactions checker. You can get to it from the forum tabs, the forum menu, as well as other links. If you just add /gp to the domain name
You will arrive there.
It is linked in the Experts Corner in the Drug Interactions category:
YMMV
20 March 2016 at 4:09 am in reply to: EMA to Review New Hepatitis C Drugs for Possible Hepatitis B Rea #14240With Hep B 95% of people who are infected as adults clear it and don’t go on to chronic Hep B
A major problem is that around the world, most of the people with chronic Hep B contracted it at birth or early childhood when their immune systems are weak and the clearance rate is <10%
With Hep C only 25% clear it and most go on to chronic Hep C
Hep C can be cured because it does not integrate itself into host cells. Hep B is a DNA virus and this DNA can form cccDNA - covalently closed circular DNA - in the nucleus of infected cells. What that means in english is that it can hide in a bullet proof dormant form.
Anybody who is HBV surface Antigen positive or has an HBV viral load should be treated with entecavir at the same time as DAAs or the the HBV will probably flare.
People with evidence of past infection who have cleared (negative surface antigen, positive core and surface antibodies) probably just need watching.
YMMV
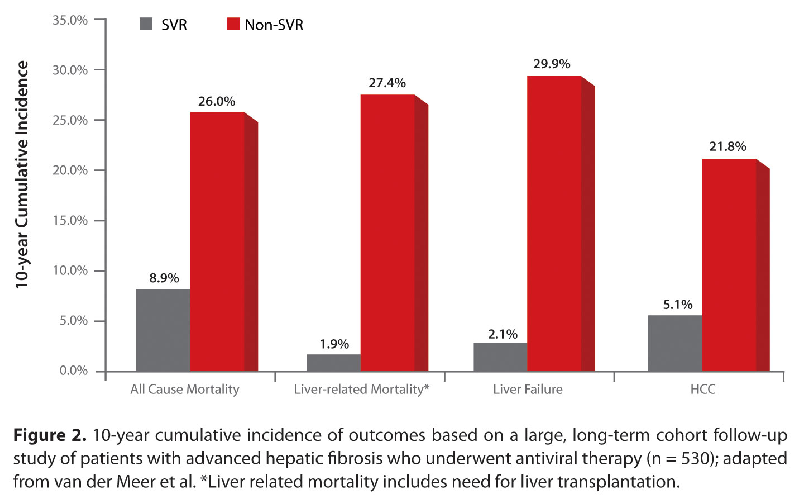
19 March 2016 at 11:20 am in reply to: Impact of Sustained Virological Response in Hepatitis C Therapy #14179 -
AuthorPosts