
Forum Replies Created
-
AuthorPosts
-
Hi Meg,
With Harvoni and your profile – 1b, naive, low fibrosis, low viral load (<6 million) the evidence is that 8 weeks treatment is just as effective as 12.
You could do 12 for insurance/reassurance, but you fit the shorter treatment profile and using it would save you $500
YMMV
So my contact form request came back with this response. My French must have been terrible because they wrote it in English!
Anyway http://bekerhepc.com is directly from Beker Laboratoires and Sofosled is a real product.
———- Forwarded message ———-
From: Sofos Hotline
Date: 19 May 2016 at 22:08
Subject: Website Laboratoires Beker & Bekerhepc.com
To: help@fixhepc.comDear Sir, Madam,
I am writing to you as per a request that was forwarded to me by our team following a post on your forum.
I wanted to certify to you that the website Bekerhepc.com is part of Laboratoires Beker. I have actually mentioned it to our IT team so that we can link them together so that it will be easier for patients to have access to all information as well as add Sofosled in our drug portfolio as it wasn’t there apaprently.
We are aware that our team members have been posting on patients forum the information about the plateform as it is fairly new.
You can also follow us on twitter @labobeker or on facebook for more information
Please do not hesitate to ask us any questions you might have on us, the plateform, the website or the treatment.
Looking forward to hearing from you!
Kind regards
Beker Team
YMMV
The Huffington Post article does not have an image to go with it.
If you go here you will find a shareable version with a good image: https://www.facebook.com/Fixhepc-650132571796578/
Anyone who has the time should talk generics in the comments section of this article, either on Huff Post or Facebook or both.
YMMV
Dr.Freeman, do you know wich research wich is not published yet is Greg talking about?
Yes, his, mine and other people we know.
SOF+DCV in GT1 is getting really good SVR rates of 95%+ but the same SOF+DCV in GT3 is seeing SVR rates below 90% in the 12 week patients. Looking at the kinetics we see that in GT1 SOF+DCV is as good or better than SOF+LDV, but when we compare SOF+DCV in GT1 and GT3:
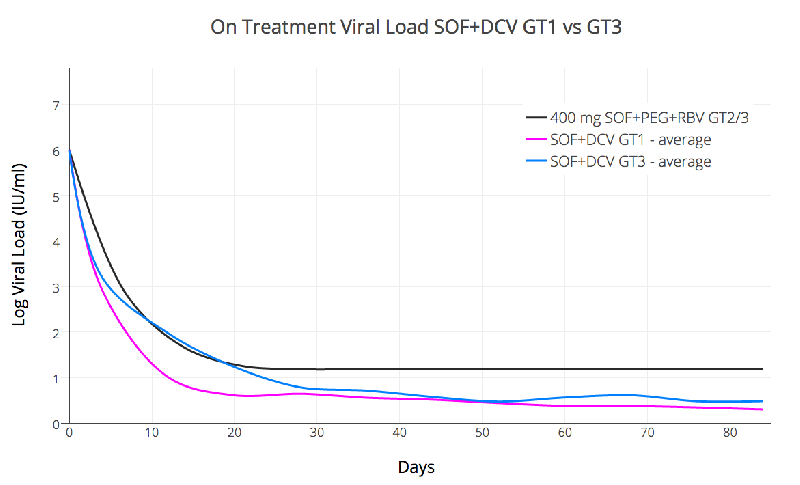
Now my interpretation of this graph is that while in GT1 we are reliably at UND by about 55 days (giving a 30 day over-treat) this is not the case in GT3 which decays much slower. This slower decay suggests longer treatment is required if we want the same insurance over-treatment buffer we have in GT1.
The sad reality is that the current DAA agents are worst in GT3, and Ribavirin does not seem to help much (if at all), so in the absence of better what we have for the moment is LONGER (or adding in Interferon and Riba)
I know people don’t like to hear it but for some low fibrosis/low life impact GT3 patients waiting for better agents is a perfectly sane option, as is treating for a bit longer than current guidelines suggest for F0-F2
YMMV
Using the contact form is a worry, it throws an error.
YMMV
Hi Kevin,
Thanks for the research. I have asked directly.
YMMV
Great news Hope. I am now cured and I took Chinese Sof/Led!!! Luckily I had a very good GP who was incredibly supportive. Keep on keeping on


YMMV
Great news Tweakmax…..those results are a carbon copy of mine at SVR12
The time will fly by…… 
YMMV
Great news Matt. Now for the journey to a cure!!
YMMV
Although the prices are higher than other options it’s good to see the idea of access by personal importation starting to take root.
YMMV
My fasting glucose level has shot up to 11.9
You should be on some metformin to bring that down.
YMMV
Hi Simone,
The key questions are Genotype and Fibrosis with Viral load and other medications potentially playing a role.
Do you know these details?
There is a handy decision support tool at http://fixhepc.com/hcv where you can put in some details and it will give you the answers according to various widely accepted guidelines – it’s a kind of inst-a-expert.
Having an online consultation on https://gp2u.com.au/ would let you discuss with a doctor very familiar with the medications.
YMMV
17 May 2016 at 4:33 am in reply to: undetectable at 9 weeks sof/dac gen 3a F3 inf/rib relapsr #17341Cirrhotics respond slower.
The rise in platelets is encouraging, suggesting your portal pressures have fallen and you spleen shrunk a bit.
With portal hypertension using beta blockers looks to me to be a historical hangover. They were one of the first effective antihypertensive medications but the sides include tiredness and sexual dysfunction issues.
ACE inhibitors also work and this has been known since 1992!
http://www.ncbi.nlm.nih.gov/pubmed/1586932
And rediscovered in 2013!
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3627462/
Here is some detailed commentary on it:
http://f1000.com/prime/reports/m/6/95/
The driving issue for you is HCV. Fixing that will go a long way towards fixing the problem and preventing progression.
YMMV
Hi Bob,
I presume you stopped the Riba because of the sides. It takes 21 days to drop by half so you will have had nearly 6 weeks worth. It’s not something usual, but will certainly have done no harm. Monotherapy with any drug, even Sofosbuvir is a bad idea so don’t take it after treatment.
Given you’ve stopped it I would stay stopped secure in the knowledge you hit the virus hard at the start.
YMMV
Me being among the people that need to be careful about a HCC recurrence
A significant proportion of HCC is AFP negative so AFP testing will miss it. You, being high risk (about 30%) should also have U/S or CT or MRI.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1240033/
APF, US or Both?
The use of AFP measurement alone as a screening tool has been successful in detecting early treatable tumours in populations with a high prevalence and incidence of HCC such as Asia and Sub-Saharan Africa.28,40,41 However, the screening for HCC with AFP alone in populations with a lower incidence of HCC is associated with very low predictive values.42,43 Trials in China have shown that the combination of US and AFP is better than either alone for the screening of HBsAg positive subjects; otherwise, US alone is the method of choice since it is better than AFP.44,45
The superiority of US to AFP was further demonstrated in a 7-year prospective surveillance study to determine the optimal test for detection of early HCC. It studied both AFP and US and concluded that US examination was more accurate than AFP. Thirty-one cases of HCC were detected in 602 patients with chronic viral hepatitis; the positive predictive value (PPV) for AFP to detect HCC was only 12% or less for all AFP cut-off values, and the maximum joint sensitivity and specificity were approximately 65 and 90%, respectively. Abdominal US on the other hand identified all 31 cases of HCC. The PPV for US examinations to detect HCC was 78%, while the sensitivity and specificity were 100 and 98%, respectively.45
YMMV
-
AuthorPosts