
{kind=link}

Super User
Lismore Liver Clinic Now Able To See Patients
Lismore Liver Clinic is now able to accept referrals for assessment and monitoring of patients accessing generic medications for the treatment of hep C.
Please note that this does not represent an endorsement of the use of generics, but rather an acceptance that if patients are doing this expert monitoring is within their scope of practice.
The clinic does not assist patients with access to generic HCV medications.
LLC accepts patients living in the NNSWLHD area which basically means south of the QLD border as far as Grafton and inland as far as Tenterfield.
The referral details are:
Lismore Liver Clinic
Level 1, 29 Molesworth Street
Lismore NSW 2480
Fax 02 6629 4633
Testing Provisions Patient Safety
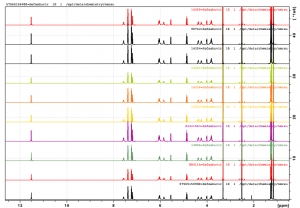
So what is this image? It is a patient safety check. Each coloured line represents a single patient's self imported Sofosbuvir being tested against a reference standard. Yes it's just lines but for each chemical there is a unique NMR signature represented by the spikes in those lines, but let's rewind.....
Back in February when patient zero asked me to help them personally import Hepatitis C medication the conversation went like this:
- Have you heard about the new DAA medications that cure Hep C?
- No, I thought the cure was worse than the disease, but it sounds interesting I'll look into it.
- Ok, so there is a cure, but it's not available (I had some Indian doctor friends check)
- Ok, so now it is available but it's the wrong treatment for you
- Ok, so you've found a supplier in China that makes what you need...
- Ok, so here's the deal:
- I will prescribe it so you can import it
- It comes to me first
- I will arrange to get it tested for you
- If it passes testing you can take it, if not I will bin it
- Ok?
- Yes
So the medication arrived, it did pass testing, patient zero took it and at 4 weeks the pathology company rang up to say:
- We think there is a problem with patient zero
- I thought OMG, I've killed him, he's in liver failure, I'm going to be in so much trouble, but said...
- Ok, so what's the problem?
- We think you've switched the blood samples because he used to have Hep C and terrible liver function tests but....
- Now his viral load is zero and his liver function is normal
- Hallelujah
- Yeah, no worries, that's expected, he's on treatment
- Oh, we don't see many of these...
So patient zero was really supposed to be a one off and was in fact sworn to secrecy, something he honoured.
The problem was I had asked some expert doctors for their opinion, and when patient zero hit VL=0 they started sending me patients who faced the options of parallel import, interferon or death.
So one patient became several, and several became more. With each passing week more people saying "I'm better" and the validation of VL=0.
While the initial testing was robust the lab that did it was careful to inform us that they were not NATA accredited to do testing, so with that in mind we went in search of a NATA accredited lab.
These APIs have also been cross checked in Australia by the NMI (National Measurement Institute) which is NATA (National Association of Testing Authorities) accredited to perform testing. Only the Department of Defense and NMI have NATA accreditation to perform this testing.
Australian NMI NATA Certification Sofosbuvir
Australian NMI NATA Certification Ledipasvir
Australian NMI NATA Certification Daclatasvir
If you happen to be a laboratory looking for real NMR data in multiple solvents, 1H, 13C, 2D, here it all is in one place:
The Trans-Pacific Partnership: the dirtiest trade deal, you've never heard of
So last night the TPP got the nod in the US. So what is it and what does it mean?
It's supposed to be a free trade agreement, but it apparently has some catches, particularly around medications and patents.
Sadly it's actually impossible to know what it means because to date it's a largely secret deal.
Before it gets the full nod it will need to be approved by our parliament. Then at least it won't be secret.
Depending on the wording it could have an impact on things like FixHepC.
Here's a video about the TPP from Get Up! Click the link to read about it on their site.
Patient Rights vs Patent Rights
The thing with Hep C is that it's not about anonymous statistics, it's about real people. Here's the story of one patient, and his wife's journey through Interferon and failure and then to self initiated treatment and cure via the parallel import of generic DAA medications that was published in the Sydney Morning Herald and The Age:
Here is a letter to the editor that did not make the cut
Sunday 27th September 2015
Dear Editor
(Ref: Hepatitis C drug buyers club aims to set up new source of support)
In 1961 JFK uttered the immortal lines "ask not what your country can do for you - ask what you can do for your country".
With the passage of time, the idea we should all put something back in seems increasingly lost.
We have at our fingertips the tools to rid the world of Hepatitis C and are separated from that only by corporate avarice.
Gilead Sciences are asking for more than the entire annual PBS medications budget, used to treat all Australians for all diseases, to treat a single disease forecast to kill half as many people as breast cancer by 2030.
If this medication pricing trend continues unabated you can foresee the day we invent a cure for cancer, but people still die because only a fortunate few can afford access.
Parallel importing is a tool that has been used before to level the playing field, most notably around the pricing of HIV medications. $1000 a tablet for something that costs $1 to produce and is available overseas for $10 does not make sense.
It’s time to draw a line in the sand and make it clear patient rights deserve equal protection to patent rights.
Kind Regards
Dr James Freeman
The Minimum Cost To Cure Hepatitis C - Revisited
A patient posted a link that contained a powerpoint presentation from Dr Andrew Hill, PhD. I asked Dr Hill if I could post it here and he said yes.
I turned that into a very quick YouTube movie, so you will probably have to pause it to read it. The attachments include the original PPT (and a PDF version) and two recent papers. Use the readmore to get to them.
FixHepC In The News
A story about the genesis of this initiative titled Big pharmaceuticals and the Hepatitis C drug trail dubbed a 'miracle cure' ran this morning in The Sydney Morning Herald and The Age.
There is also another story in the Sydney Morning Herald specifically about the FixHepC Buyers Club called Hepatitis C drug buyers club aims to set up new source of support.
Hep C drugs queue just gets longer
Hepatitis Australia is using new data released from the Kirby Institute today showing only one per cent of people with hep C received treatment last year to push the government to list new hep C drugs without delay.
"It's time for action," said Kevin Marriott, Hepatitis Australia Acting CEO. "It's time of the federal government to make new therapies widely available, increase liver clinic capacity, upscale hepatitis C treatment and prevention programs and transform the lives of thousands of Australians."
New surveillance data from the Kirby Institute estimated some 230,470 people had chronic hepatitis C infection at the end of 2014. Around 80 percent had early to moderate fibrosis and 19 percent had severe fibrosis or hepatitis C related cirrhosis.
The estimated number of people with severe liver disease/hepatitis C related cirrhosis has more than doubled in ten years, according to the data.
Head of the viral hepatitis clinical research program at the Kirby Institute Professor Greg Dore said that without significant improvement in hepatitis C treatment rates, Australia would see a 245 percent increase in the rates of liver cancer and 230 percent increase in hep C-related deaths by 2030.
"Thousands of Australians are queuing up waiting for new medicines to be PBS listed. These treatments provide one of the great breakthroughs in clinical medicine in recent decades, with enormous potential to improve the lives of people living with hepatitis C," Professor Dore said.
Four new hep C medicines - Gilead's Sovaldi (sofosbuvir) and Harvoni (ledipasvir/sofosbuvir), BMS's Daklinza (daclatasvir)and AbbVie's Viekira Pak (paritaprevir with ritonavir, ombitasvir and dasabuvir plus ribavirin) - have been recommended for PBS listing but price negotiations with sponsors are ongoing. Professor Dore said previously, he suspected listing is more likely for sometime in 2016.
Mr Marriott said there is compelling evidence for the new medicines to be listed without delay before people progress to serious liver disease and die.
"Interferon-free therapies will allow the vast majority of people living with the hepatitis C virus to be cured, even where treatment has failed previously and without the terrible side-effects of existing treatments."
Michelle Lam
Originally published in Pharma in Focus. Reproduced with permission.
Hep C Buyers Club In TGA Sights
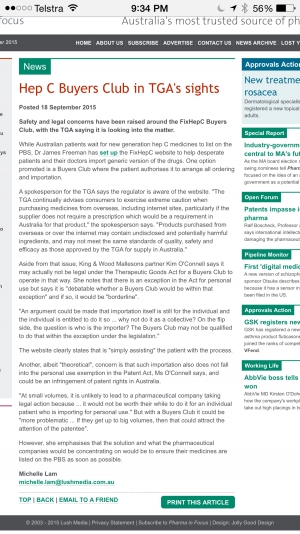
It has always been a worry that the powers that be may not like the idea of patients parallel importing life saving medications.
The Buyers Club has been active for less than 24 hours and already it seems the battle lines are being drawn: http://www.pharmainfocus.com.au/
The TGA has a job to do, and that is to ensure the medications available to Australian's are safe and useful. Why they let Chemist Warehouse sell bottles of water and call them homeopathic melatonin is beyond me but that's another story.
My job as a doctor is to treat patients with medicines that work.
I'm hopeful that the TGA will continue to respect your personal right to source medication from places where it is available at an affordable cost, rather than abuse its power to prevent that.
This could turn out to be the first big crisis for the Turnbull government - protect the interests of Gilead or those of ordinary Australians.
We will keep you posted as updates come to hand.
PBAC 2015
In the last blog reference was made to the failed 2014 PBAC submission, simply because I could not find the PBAC outcome. Somebody has been kind enough to flag my attention to the PBAC 2015 recommendation papers which you can read here:
- http://www.pbs.gov.au/info/industry/listing/elements/pbac-meetings/psd/2015-03/sofosbuvir-sovaldi-psd-03-2015
- http://www.pbs.gov.au/info/industry/listing/elements/pbac-meetings/psd/2015-03/harvoni-ledipasvir-sofosbuvir-psd-03-2015
Sadly the original analysis still largely holds. In no particular order, here are some key points for patients to consider.
Rationing
Treatment criteria: Must be treated in an accredited treatment centre.
So the same Hep C clinic waiting list system will continue.
Patient Treatment Targets
6.26 The PBAC recalled that for the submissions for boceprevir and telaprevir the ICER range presented for a time horizon of 30 years was $15,000/QALY - $45,000/QALY. The PBAC noted, though the prevalent CHC population was approximately 230 000 patients, that approximately 60 000 patients could be treated within the estimated health system capacity over 5 years
Here is a table of the targets:
|
Year 1 |
Year 2 |
Year 3 |
Year 4 |
Year 5 |
|
6,600 |
9,900 |
15,000 |
15,000 |
15,000 |
With over 10,000 new infections a year we don't even make headway until year 3 at which stage we will only be reducing the number of people with Hep C by 5,000 a year.
Harvoni will only be for GT1 and for all other Genotypes Sovaldi is approved for use with PEG/Ribavirin or Ribavirin
The proposed treatment regimens for patients with different genotypes
|
Genotype |
Treatment duration |
Treatment regimen |
|
Treatment-naïve (no prior treatment with interferon) |
||
|
1, 4, 5, 6 |
12 weeks |
SOF12 + PR12 |
|
2 |
12 weeks |
SOF12 + R12 |
|
3 |
12 weeks |
SOF12 + PR12 |
|
24 weeks |
SOF24 + R24 |
|
|
Treatment-experienced (prior therapy with an interferon based regimen) |
||
|
2 |
12 weeks |
SOF12 + R12 |
|
3 |
12 weeks |
SOF12 + PR12 |
|
24 weeks |
SOF24 + R24 |
|
Price
Although PBAC have redacted some numbers they have not redacted enough:
1.1 Taking account of the proposed drug prices, treatment targets in the Fourth National Hepatitis C Strategy and assuming that care continues to be delivered through specialist treatment centres, DUSC estimated the following number of patients of all genotypes would be treated over the first five years of listing at a net cost to the PBS/RPBS of approximately $3 billion over five years.
Over 5 years, it is estimated that approximately 61 500 patients would be treated....
So the whispers of France's 41,000 ($65,000 AUD) price appear correct - it's at least $50k a patient to take 61,500 over 3 billion.
Patient Subsidy Scheme
Here's a thought.
Rather than fund this through the PBS if the government gave patients $1/2 a billion in direct subsidies (@$2000/head) we could treat everyone in the community using generic imports and GPs to make it happen. At that point we would have effectively no hep C in the environment, new infection rates would fall towards zero because IVDUs would struggle to find an infected needle to share, and as a country we would be $2.5 billion dollars better off.
We could almost put an end to Hep C by this time next year.
We should have massive factories making this stuff and distribute it like polio vaccine - to everyone, everywhere.
How about it Malcolm? Now that would really be leadership...
PBAC, the PBS and Rationing
 In Australia there has been optimism about the PBACs decision to recommend that Hep C treatments are put on the PBS.
In Australia there has been optimism about the PBACs decision to recommend that Hep C treatments are put on the PBS.
Some people seem to think that what this means is that these new medications may well be widely available at affordable prices.
Sadly that is unlikely to be the case, for a number reasons, but first a bit of background.
To get a new drug to market a drug company needs to find it, and then test it in various ways. Testing progresses through a number of stages until there is enough confidence to test it in humans through phase 1, 2 and 3 trials. At each stage more people take the medication. Once the trails conclude the drug company goes to the regulator and says "here is the evidence it works, we now want to sell it". If it all stacks up the regulator - TGA, FDA, EMA, etc grants what is called "marketing approval".
At this point the drug company starts advertising it to doctors and a doctor can write a script for it. Prices are typically very high as the drug company tries to recoup their development expenses.
Many countries have various forms of medication subsidy programs to provision access to expensive medicines for patients that could not afford to pay for them themselves.
The PBAC and The PBS
In Australia our medication subsidy program is called the Pharmaceutical Benefits Scheme (PBS). Getting a medication listed on the PBS is something of "The Holy Grail" for a drug company because now they can continue to charge a high price but the patient pays a much lower price and the PBS pick up the balance of the cost. In the the 2013/14 financial year PBS medication cost $8,837,605,701 with the Government paying $7,292,550,961 (83%) and patients contributing $1,545,054,740 (17%)
http://www.pbs.gov.au/statistics/2013-2014-files/tables-2-2a.pdf
To get on the PBS a drug company needs a recommendation from the Pharmaceutical Benefits Advisory Committee (PBAC) so the conversation goes like this:
Big Pharma: "Hey we've got this great drug it does this...."
PBAC: "Great, how much is it?"
Big Pharma: "Well you will save $X so we think $X x 90% would be fair"
PBAC: "You're dreaming, sharpen your pencils and come back when you're serious"
Now this cycle of price negotiation proceeds slowly because the PBAC only meets 3 times a year.
Looking at Hep C drugs we've seen this happening and the PBAC has decided that the price has been reduced enough that the cost-benefit analysis stacks up.
A more in depth analysis of this process is here on http://theconversation.com/why-medicines-take-so-much-time-to-get-listed-on-the-pbs-10902.
So what happens next?
First a firm price needs to be agreed. Rumour has it that price will be France's 41,000 Euro price (currently around $65,000 AUD). To treat all 233,000 Australians with this medication at that price would see a bill of around $15 billion. That's around twice what our Government spends on all the medications subsidised by the PBS each year so do the political math about a Government on the one hand saying "Hey we need a co-pay to save $1 billion", and on the other, "but we want to spend $15 billion over here".
Anyway a positive PBAC recommendation goes to Cabinet for the yay or nay.
Not everything gets the nod at Cabinet, but let's simply assume it does. What will that PBS approval look like for patients?
Not great is the answer, because it will be rationed.
These medications are simply way to0 expensive not to ration and everything else on the PBS at similar price points is heavily rationed.
Here is the rejected PBS application (the one that got the PBAC nod is not, as far as I can find, published yet):
http://www.pbs.gov.au/industry/listing/elements/pbac-meetings/psd/2014-07/sofosbuvir-psd-07-2014.pdf
1 Purpose of Application
1.1 Section 100 (Highly Specialised Drugs Program), Authority Required (STREAMLINED) listing for sofosbuvir for the treatment of chronic hepatitis C (CHC) in the following populations:
- Treatment naïve, Genotype 1-6;
- Treatment naïve, Genotype 1-3 in patients unsuitable for treatment with interferon based therapy;
- Treatment experienced, Genotype 2 and 3; and,
- Treatment experienced, Genotype 2 and 3 in patients unsuitable for treatment with interferon based therapy.
1.2 The submission had not requested listing for genotypes 4, 5 or 6 treatment naïve patients who are unsuitable for interferon (IFN) therapy, nor for genotypes 1, 4, 5 or 6 for patients who are treatment experienced.
There are a series of take home points from this:
- Gilead's earlier application excluded a lot of patients
- Once you progress past section 1 you will see further exclusions like "Patient must have compensated liver disease"
- This is an S100 application and that in itself restricts access even further
So what is S100?
When a medication is listed on the PBS it can be in any of the following broad categories (there are some further nuances I'm ignoring):
- General benefit - anyone can have it, any GP can prescribe
- Restricted benefit - anyone with a certain condition can have it, any GP can prescribe
- Authority required - anyone with a certain condition can have it, and for most (but not all) a GP can still prescribe it but:
- Government approval is required
- Streamline (done by software)
- Phone (requires a doctor to call and ask for permission)
- Government approval is required
- S100
- Like a phone authority where only patients who meet the criteria can have it, but with the added kicker that.....
- Only a small group of doctors with formal S100 prescriber rights for that medication can prescribe it
A cynic would call this rationing by stealth.
Hep C and HIV are similar so let's look at HIV medication to see what a PBS listing is likely to look like.
Here is an indication of what the doctors need to do to be able to prescribe S100 HIV medications: http://www.ashm.org.au/hiv/prescriber-programs.
And here is the wording on the restrictions for prescribing a common HIV medication called Atripla (Also a Gilead product) when it was first listed http://www.pbs.gov.au/info/industry/listing/elements/pbac-meetings/psd/2011-11/pbac-psd-tenofovir-nov11
Restriction: Section 100 listing
Public Hospital Authority Required (STREAMLINED)
Private Hospital Authority Required
Initial treatment of HIV infection in combination with other antiretroviral agents in a patient with a CD4 count of less than 500 per cubic millimetre or symptomatic HIV disease;
Continuing treatment of HIV infection in combination with other antiretroviral agents where the patient has previously received PBS-subsidised therapy of HIV infection.
Now you can buy Atripla privately for $1186.39 for 30 tablets from Chemist Warehouse so it's at least 20 times cheaper than Harvoni, so you could reasonably expect it to have less restrictions on its prescription. In fact, that has happened, because the restrictions around CD4 count have been removed since the original recommendation back in 2011.
So what does it all mean?
Even when the new Hep C medications are PBS listed the chances are better than fair that you personally won't be able to get them because either a) you won't be eligible or b) you won't be able to see an approved S100 prescriber who might reasonably be expected to be the same people running the Liver Clinics and maybe Gastroenterologists and Infectious Disease Specialists being "grandfathered in" without any special training. That's the typical approach.
As time passes, prices will fall, and the rationing will be eased, but even at the $1186 a month price point for medications like Atripla significant restrictions continue to exist.....
You would have to be a rampant optimist to believe historical PBS listing practices will not be applied to Hep C medications.
That's not to say you should not, or cannot afford to wait. It is to say that if historical patterns are followed, for most people, waiting years to access treatment is going to be inevitable.
If it was me I know what I'd do, but everybody is different and YMMV.