
Home › Forums › Main Forum › Experts Corner › Resistance › Highly detailed article on DAA resistance
- This topic has 13 replies, 9 voices, and was last updated 9 years, 9 months ago by
 isaing4.
isaing4.
-
AuthorPosts
-
31 August 2016 at 7:23 am #2267231 August 2016 at 12:04 pm #22674
That’s very complex for a bear of little brain like me
Genotype 1a
Diagnosed in 2004, had HCV for all my adult life. Until 2016!!!!
Harvoni treatment, started 19 March 2016
4 week results Bilirubin 12 down from 14 pre treatment,
Gamma 25 down from 52, ALT 19 down from 63, AST 19 down from 47,
VL <15 down from a lazy 6 million or soEOT Results
Bilirubin 10, GGT 18, ALT 19, AST 21, VL UND12 Weeks post EOT
Bilirubin 11, GGT 16, ALT 22, AST 20, VL UND
Cured baby31 August 2016 at 7:29 pm #22686Thanks for posting Doc. Will download and read with interest!
1 September 2016 at 10:40 am #22711Thanks again Dr Freeman for another in depth article. I’ll have to read that one in the morning when my brain is firing on all cylinders!

G1a dx’d in 1992, Biopsy F2 VL 8mill +. Tried tx with Interferon/Riba, back in 2008 didn’t last long it felt horribly ugly!! I stopped tx, after 5 weeks!!
Started tx 6/1/16 with Harvoni.
12 Month Labs= UND1 September 2016 at 11:34 am #22717I’ve been reading so far 1/3rd from this interesting, yet challenging material. (Doctors use a complicated language
 , no ofense dr. F)
, no ofense dr. F)It is like talking about a microuniverse (well in fact it is like this) with different rules and some science fiction stuff… A Star Wars, with rebels and clones…. I look forward to read the rest of the material and see who in the end will have “the force”.
Cheers,
RHF
In fiecare an HCV ucide peste 500000 oameni.Medicamentele generice pentru hepatita C functioneaza. Nu deveni statistica! Cauta pe Google “medicamente generice pentru hepatita C”.
HCV kills more than 500000 people every year. HCV generic drugs work. Don’t become a statistic.
By sharing this Youtube video you might save someone’s life!
My TX: HEPCVIR-L[generic Harvoni]-India
SVR52 achieved1 September 2016 at 1:35 pm #22723Thanks Dr Freeman, wow that is a lot of info to attempt to digest. Could be a problem for the likes of me with a particularly unscientific mind but will try to go through it all slowly. It is like a foreign language of its own!
Just gleaning a little of it I hope it will further assist the specialist to pin point the correct treatment for each individual but it does look unbelievably complex!!!!!! Guess there is always more and more to learn about this tiny yet vicious virus!
Diagnosed Hep C genotype 1b early 1990’s. Treated 1998 peg Interferon/Riba non responder
 ( Meds stopped after 4 or 5 months.
( Meds stopped after 4 or 5 months.
Fibroscan April 2013- 7.3kPa repeated May 2015- 5.8kPa mild scaring
May 2015 ALT 59 AST 56
21/7/2016 ALT 36 AST 44 BIL14
VL 939000
thanks FixhepC +Monkmed started Sof/Led 16/8/2016.)
OCT 3 AST33 VL UND
OCT 11 ALT 29 AST 36 VL UND
NOV 10 ALT 27 AST 37 VL UND
JAN 30 2017 ALT 23 AST 29 VL UND
SVR12 ALT 23 AST 27 VL UND!!
SVR 24 UND!!!TY EVERYONE!6 September 2016 at 4:46 pm #22816Just finished reading the article
 .
. I’ve reached the point to have a better understanding about why some patients do relapse and what these Resistant Variants are.
From the perspective “risk of developing Resistant Variants”, I would say it is quite tricky to treat HCV for 8 weeks only (as Gilead is doing for non-experienced patients). I would not “play” with the duration of the treatment just for saving some money. Since the generic drugs are much much cheaper, it seems to be a non-sense to treat for a shorter duration just to save some dollars.Also interesting to see that NS5A inhibitor-resistant viruses may persist for years, potentially impairing the results of re-treatment…. This should be deeper thought and discussed with the doctor in case of a relapse, as just buying the same medicines for another course of treatment for “12/24 weeks” might not be enough.
……
In fiecare an HCV ucide peste 500000 oameni.Medicamentele generice pentru hepatita C functioneaza. Nu deveni statistica! Cauta pe Google “medicamente generice pentru hepatita C”.
HCV kills more than 500000 people every year. HCV generic drugs work. Don’t become a statistic.
By sharing this Youtube video you might save someone’s life!
My TX: HEPCVIR-L[generic Harvoni]-India
SVR52 achieved7 September 2016 at 12:55 am #22824I read this whilst resting after colonoscopy last week and I so had plenty of hours to read it a couple of times.
All I can say from my heart is that I am damned lucky to have responded to the Sof/led straight up and that the old tx didn’t stuff that up as well as some other parts of my little world.
Also appreciate the posts which included graphs on generic data in another recent thread. I do like stats and data and research, weirdly! Doesn’t necessarily fit my profile as a trained classical musician. Mind you we did stats at uni!
Thankyou Dr. for this link.
To those who are still finding avenues with the new meds and combos I am thinking of you all and wish all a positive outcome in treatment
A7 September 2016 at 5:04 am #22830My personal view is that the thinking on resistance is wooly.
HCV is a quasi-species meaning that it mutates pretty rapidly. Each replication cycle brings the a possibility of roughly 1:10,000 of creating a mutant. Once this is created it exists. If it can’t reproduce it dies. If it can, and it is resistant then it will take it’s place in the population according to its fitness. If it is very fit we may be able to see and measure it (fit means makes lots of kids fast), but if it is less fit we won’t be able to see and measure it.
THE FACT THAT WE CAN’T SEE ENOUGH TO MEASURE DOES NOT MEAN ITS NOT THERE!
The key point is the the CREATION of resistance requires replication, so it happens BEFORE treatment starts unless we don’t get good viral suppression and replication continues.
When we treat we kill of the easy to kill virus and suppress almost all replication. With no replication there is no opportunity for a mutation to form.
Virus that already existed, that is resistant will not be killed efficiently, although it’s growth will not be helped by the drugs. Nevertheless it will survive and when we remove the drugs it grows back. Now we can see it and measure it, but it was not created by treatment. It existed before we started.
In HIV we know that resistance occurs in the context of ongoing replication.
http://www.ncbi.nlm.nih.gov/pubmed/19048205
HIV is an unstable RNA virus like HCV so the lessons there apply here. And the lesson for retreatment should be hit the virus as hard as possible to suppress replication (ie add Riba and or a 3rd DAA) so that an already partly resistant virus can not add more resistance mutations to the same strand of RNA.
Anyway those are my thoughts. I expect conventional wisdom to catch up in due course. As you can see from the abstract above this idea is known, it just does not seem to get talked about much in HCV circles.
The reason for waiting to retreat is, to me, not to wait for RAVs to fall to levels we can’t measure. They will still be there, probably forever. It is to wait for access to more powerful drugs, or preferably extra agents
The advantage of a 3rd agent
RAVs deliver a 10x 100x or even 1000x resistance to drugs. What this means is that the EC50 (Effective Concentration to kill 50%) of a better drug needs to be 10x + to make a real difference. Let’s look at GT3 EC50:
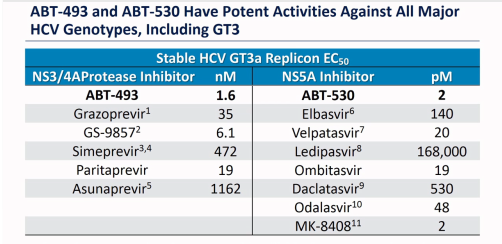
We can see for example that Velpatasvir needs 20 pM to get to EC50 and Daclatasvir needs 530 pM so VEL is 26.5x more potent than Dac. However this is in a test tube. 75% of VEL is excreted unchanged in faeces so it is possible it’s not absorbed (the literature speculates on this). That might well reduce the 26.5x to more like 7x. Anyway if you look at the potencies you can see that even for the best in class ABT-530 (that you can’t get) it is at best 250x better than DCV. This is good, but still leaves the 1000x resistance variants as problem children.
Ok, now consider a 3rd good drug.
If the probability of creating 1 resistant variant is 1:1000 (it’s lower than this but let’s use this) the probability of getting 2 resistance variants in the same bit of RNA is 1:1000 x 1:1000 which is 1:1,000,000. Now if we add a 3rd agent the virus now needs to have 3 resistance sites in the same strand of RNA and the chances of getting that are 1:1000 x 1:1000 x 1:1000 or 1 in a billion. Notice that the extra drug adds what you might call 1000 units of power, whereas even the best most potent new drug add 250x
Conclusion: 3 drugs beats 2 drugs.
Validation: In HIV we start with 1 drug: AZT and it works but resistance is rapid. Then we get ddI and ddC
http://www.ncbi.nlm.nih.gov/pubmed/19048205
And we find that 2 drugs beats 1 drug. And nowadays with lots of agents HAART (Highly Active Antiretroviral Therapy) with 3 or even 4 agents is the standard of care.
HCV is an RNA based virus like HIV. Yes it does not have a reverse transcriptase but the core genome is RNA so lessons from HIV are broadly applicable.
Validation2: Viekira-pak is a very effective existing poly target treatment, and as the QUARTZ-1 trial shows adding Sofosbuvir to it makes it outstanding. C-SWIFT is adding SOF to Zepatier’s NS3/4A + NS5A combination.
YMMV
7 September 2016 at 6:58 am #22835Thanks Doc!
I am not a medical person and lots of this information just does my head in,but I think understand the big picture.
Please correct me if I am wrong, but in my case say if I test positive again (and the chance of re-infection is pretty damn tiny), there should be enough drugs to treat (i.e. destroy without mercy) the mutants that were not destroyed in the first place.
Thanks
Genotype 1a
Diagnosed in 2004, had HCV for all my adult life. Until 2016!!!!
Harvoni treatment, started 19 March 2016
4 week results Bilirubin 12 down from 14 pre treatment,
Gamma 25 down from 52, ALT 19 down from 63, AST 19 down from 47,
VL <15 down from a lazy 6 million or soEOT Results
Bilirubin 10, GGT 18, ALT 19, AST 21, VL UND12 Weeks post EOT
Bilirubin 11, GGT 16, ALT 22, AST 20, VL UND
Cured baby7 September 2016 at 8:04 am #22839”James-Freeman-facebook” wrote:My personal view is that the thinking on resistance is wooly.
HCV is a quasi-species meaning that it mutates pretty rapidly. Each replication cycle brings the a possibility of roughly 1:10,000 of creating a mutant. Once this is created either it exists. If it can’t reproduce it dies. If it can, and it is resistant then it will take it’s place in the population according to its fitness. If it is very fit we may be able to see and measure it (fit means makes lots of kids fast), but if it is less fit we won’t be able to see and measure it.
THE FACT THAT WE CAN’T SEE ENOUGH TO MEASURE DOES NOT MEAN ITS NOT THERE!
The key point is the the CREATION of resistance requires replication, so it happens BEFORE treatment starts.
…..
/Hello dr. Freeman,
thank you for this answer.
Indeed, thinking on resistance might be wooly, however the “(too much) thinking on these resistants” does exist in my case.
During my IFN+RBV treatment my body could not clear the virus in the first 3 months of treatment (was able to clear it within the first 6 months of treatment). This makes me think that I was having perhaps some of these “resistant” viruses ….. Yet now with the SOF+LED treatment, my body was able to clear the virus in less than 4 weeks. So hopefully these “resistant” viruses were killed too.
At this stage however the thinking (at least my thinking) is easily slipping from the science behind the drugs to the fear of “what if … one resistant virus managed to survive?”, which is a different perspective. Well, 1 month + 1 week left till I will know the answer . Cheers,
RHF
In fiecare an HCV ucide peste 500000 oameni.Medicamentele generice pentru hepatita C functioneaza. Nu deveni statistica! Cauta pe Google “medicamente generice pentru hepatita C”.
HCV kills more than 500000 people every year. HCV generic drugs work. Don’t become a statistic.
By sharing this Youtube video you might save someone’s life!
My TX: HEPCVIR-L[generic Harvoni]-India
SVR52 achieved7 September 2016 at 11:51 am #22841”James-Freeman-facebook” wrote:The key point is the the CREATION of resistance requires replication, so it happens BEFORE treatment starts unless we don’t get good viral suppression and replication continues.
When we treat we kill of the easy to kill virus and suppress almost all replication. With no replication there is no opportunity for a mutation to form.
Virus that already existed, that is resistant will not be killed efficiently, although it’s growth will not be helped by the drugs. Nevertheless it will survive and when we remove the drugs it grows back. Now we can see it and measure it, but it was not created by treatment. It existed before we started.
The reason for waiting to retreat is, to me, not to wait for RAVs to fall to levels we can’t measure. They will still be there, probably forever. It is to wait for access to more powerful drugs, or preferably extra agents
The advantage of a 3rd agent
RAVs deliver a 10x 100x or even 1000x resistance to drugs. What this means is that the EC50 (Effective Concentration to kill 50%) of a better drug needs to be 10x + to make a real difference. Let’s look at GT3 EC50:
Conclusion: 3 drugs beats 2 drugs.
Thanks dr. Freeman for more info!
I have a question, please. What does nM respectively pM unit of measure stands for? M is mol of substance, chemistry?
However, Ledipasvir versus Daclatasvir … I was very lucky to be cured with Ledipasvir. It’s great that there are already solutions for those who have not succeeded yet, Velpatasvir and Viekira-pak.
But the results for ABT-493 and ABT-530 are even more spectacular.http://www.ncbi.nlm.nih.gov/pubmed/27456384
Good luck, good health and only UND to everyone!

HCV since I don’t know. Diagnosed in 2010.
GT1b, F0/F1, VL 9M, ALT 44, AST 42, Tx naive,
started 12 wks Twinvir on 06.12.2015. Feeling great and grateful 🙂
virus not detected 06.02.2016 & SVR24
isaing4@gmail.com7 September 2016 at 1:05 pm #22842Hi isaing4,
I believe the units of measure are nano-Mol and pico-Mol.
But note that chart is only for genotype 3a which is why Ledipasvir looks so bad in comparison and that is why it isn’t used for 3a. Ledipasvir would look much better on charts for 1a or 1b and works fine there as you’ve proved.

G3a since ’78 – Dx ’12 – F4 (2xHCC)
24wk Tx – PEG/Riba/Dac 2013 relapsed
24wk Tx – Generic Sof/Dac/Riba 2015/16 relapsed
16wk Tx – 12/01/17 -> 03/05/17 NS3/NS5a + Generic Sof
SVR7 – 22/06/17 UND
SRV12 – 27/07/17 UND
SVR24 – 26/10/17 UND
7 September 2016 at 5:42 pm #22844Hi Gaj,
You are right, chart for GT3 where Ledipasvir is x1000 less effective compared with Daclatasvir!
Tiny quantity of active substance

1 Mol = 1 M = 6.02 x 1023 moleculesand in the chart are nM = 10-9 or pM = 10-12
Thanks for the explanation!
HCV since I don’t know. Diagnosed in 2010.
GT1b, F0/F1, VL 9M, ALT 44, AST 42, Tx naive,
started 12 wks Twinvir on 06.12.2015. Feeling great and grateful 🙂
virus not detected 06.02.2016 & SVR24
isaing4@gmail.com -
AuthorPosts
- You must be logged in to reply to this topic.